Articles
- Page Path
- HOME > Perspect Integr Med > Volume 2(2); 2023 > Article
-
Original Article
Effectiveness of the Korean Medicine-Based Postnatal Healthcare Program: A Retrospective Observational Study -
Joohee Seo1
 , Doeun Lee2, Hansong Park3, Inae Youn3, Jungtae Leem4, Minjung Park5,*
, Doeun Lee2, Hansong Park3, Inae Youn3, Jungtae Leem4, Minjung Park5,* -
Perspectives on Integrative Medicine 2023;2(2):117-125.
DOI: https://doi.org/10.56986/pim.2023.06.006
Published online: June 23, 2023
1Department of Neuropsychiatry of Korean Medicine, National Medical Center, Seoul, Republic of Korea
2Department of Neuropsychiatry, College of Korean Medicine, Won Kwang University, Iksan, Republic of Korea
3Department of Clinical Korean Medicine, Graduate School, Kyung Hee University, Seoul, Republic of Korea
4Wonkwang University, Iksan, Republic of Korea
5Public Health and Administration, Seoul Digital University, Seoul, Republic of Korea
- *Corresponding author: Minjung Park, Public Health and Administration, Seoul Digital University, 424, Gonghang-daero, Gangseo-gu, Seoul 07654, Republic of Korea, Email: mjimage@hanmail.net; mj.park@sdu.ac.kr
©2023 Jaseng Medical Foundation
This is an open access article under the CC BY-NC license (http://creativecommons.org/licenses/by-nc/4.0/).
- 1,658 Views
- 36 Download
Abstract
-
Background
- Insufficient postpartum care can negatively affect mothers’ health. The aim of the Korean Medicine-based Postnatal Healthcare Program (KMPHP) is to prevent and treat Sanhupung by rapid intervention in postpartum care.
-
Methods
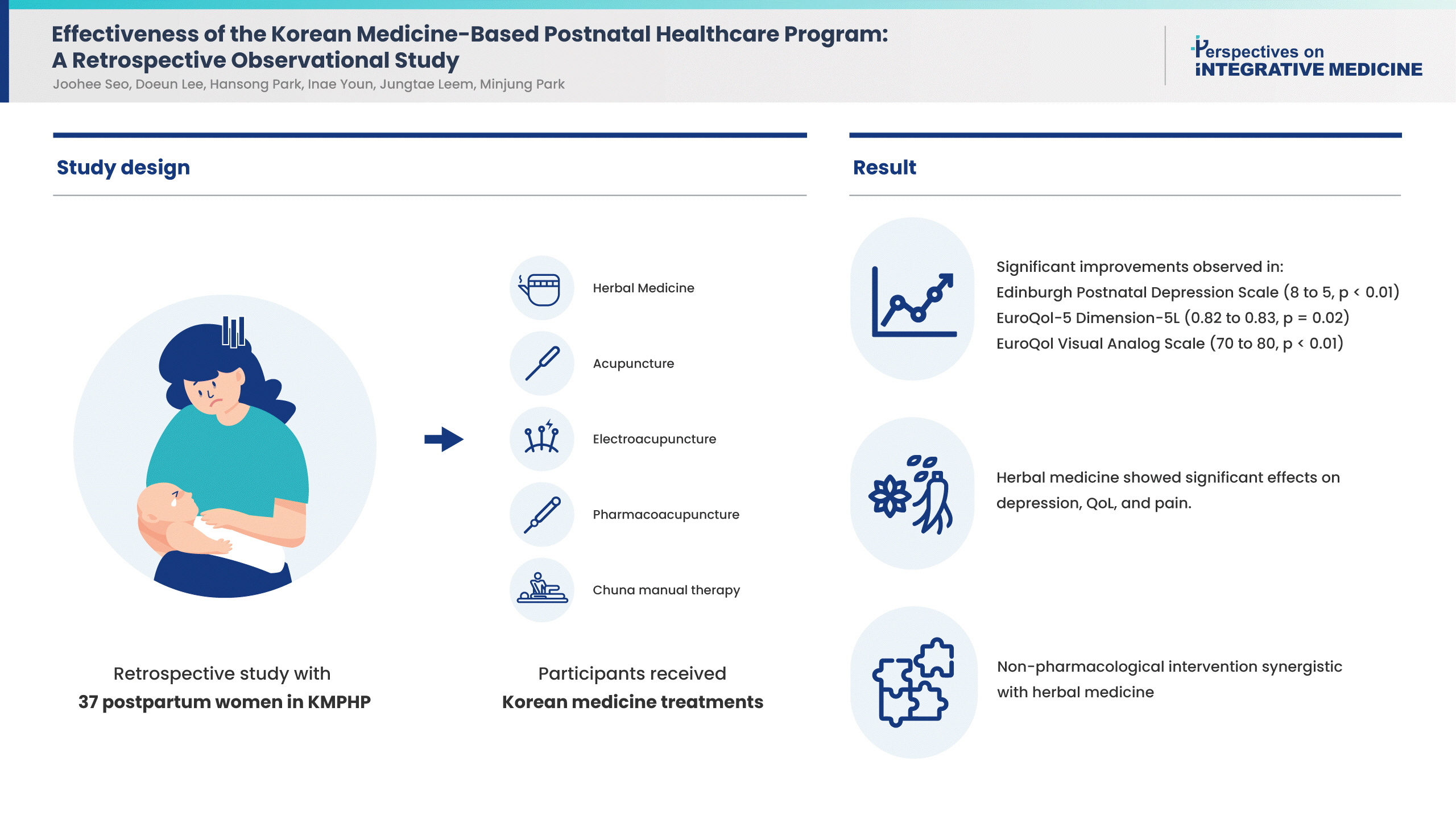
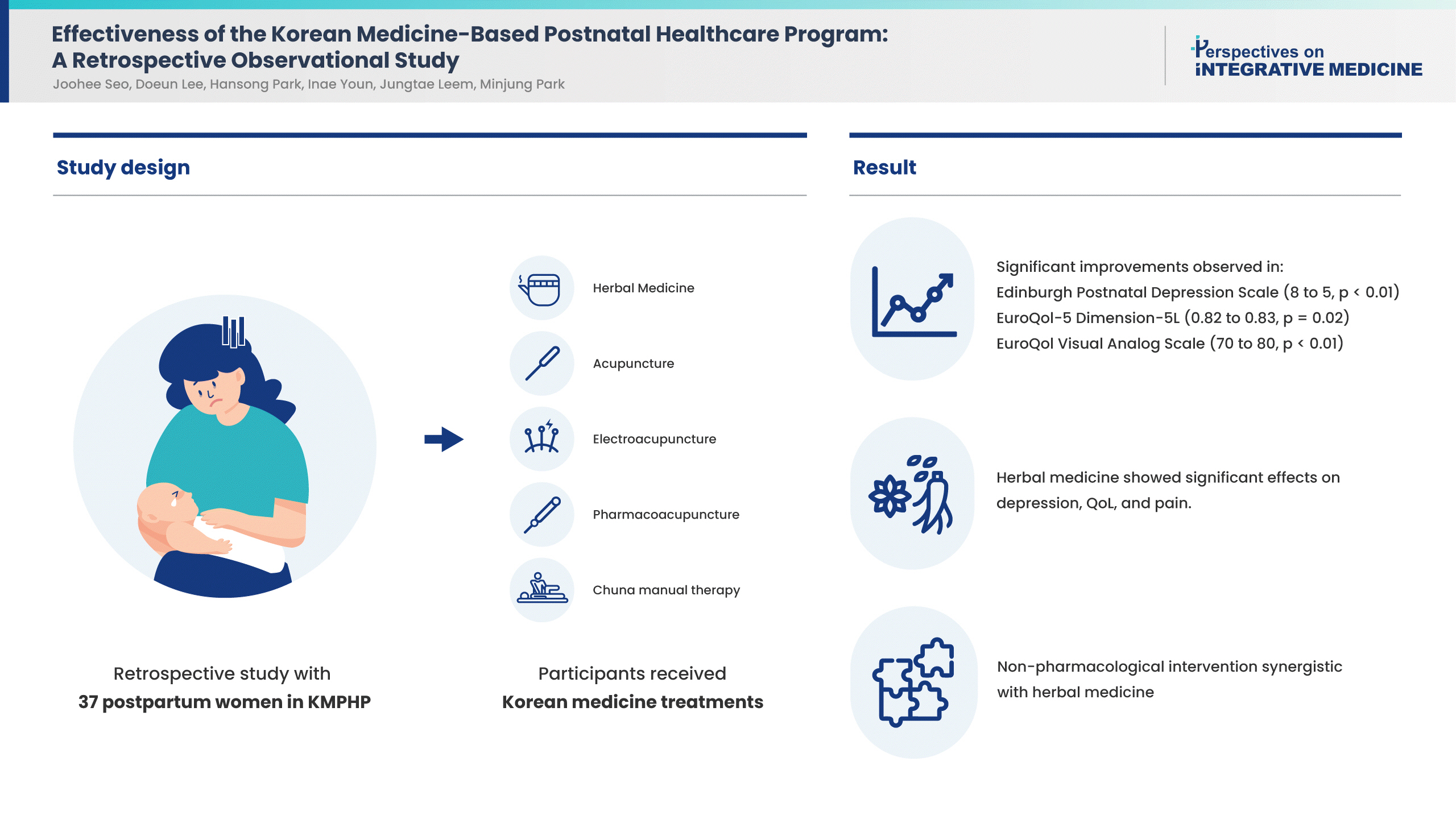
- A retrospective study was conducted using data from 37 postpartum women who participated in the KMPHP between April 2019 and April 2020. The women had received at least one type of Korean medicine treatment (herbal medicine, acupuncture, electroacupuncture, pharmacoacupuncture, or Chuna manual therapy) for at least one session. General characteristics were collected from the medical records, and postpartum symptoms (taken from a questionnaire) were investigated. Outcome measures included pain intensity, quality of life (QoL), and postpartum depression.
-
Results
- The effectiveness of the KMPHP was determined using the paired-sample Wilcoxon test and significant improvements in the scores were observed using the Korean version of the Edinburgh Postnatal Depression Scale (from 8 to 5, p < 0.01), EuroQol-5 Dimension-5L (from 0.82 to 0.83, p = 0.02), and EuroQol Visual Analog Scale (from 70 to 80, p < 0.01). The womens’ pain scores (Numeric Rating Scale) reduced from 4 to 3 after treatment, but the difference was not significant. As a result of analyzing the effects of each intervention, herbal medicine show a significant effect on womens’ depression, QoL and pain, and non-pharmacological intervention showed synergistic effects with herbal medicine.
-
Conclusion
- Korean medicine-based interventions may be effective in the management of postpartum health by improving mothers’ emotional status, QoL, as well as reducing pain.
- The postpartum period is a critical time for women during which they undergo intensive health recovery; if poorly managed, it can lead to complications [1]. As maternal age at delivery rises, so does the number of pregnancies at 35 years and above, high-risk pregnancies, and multiple pregnancies due to increased numbers of in vitro fertilization, which can necessitate professional interventions in postpartum health management [2]. Western medicine for postpartum care has mainly focused on examining organ damage in various pathological conditions related to delivery and postpartum complications, pelvic floor physiotherapy, mental health, and managing reproductive health.
- In Traditional Korean Medicine theory, symptoms that manifest during the postpartum period are collectively called “Sanhupung,” and a more comprehensive medical management is emphasized during this phase [3,4]. Sanhupung, a culture-specific condition/disease associated with postpartum management, is a concept unique to Korea, and numerous studies have emphasized the importance of treating the condition/disease as it can affect a mother’s recovery [5]. As one of the major conditions/diseases caused by inadequate postpartum management, its importance is recognized not only in Korea, but in other countries such as China [6].
- Sanhupung can be largely classified into musculoskeletal, gastrointestinal, respiratory, neurological, circulatory, and psychological symptoms. Musculoskeletal symptoms (78.08%) such as bone and joint pain are the most common forms of Sanhupung, followed by neurological symptoms such as sleep disorders and depression, and circulatory symptoms such as edema [7]. Korean medicine (KM) interventions for postpartum management include acupuncture, moxibustion, dry cupping, and herbal medicine (HM), amongst others. Korean medicine doctors (KMD) prescribe individualized treatment according to the mother’s symptoms to prevent the deterioration of health which may occur in the absence of appropriate postpartum care [8].
- Recently, several local governments in Korea have initiated HM supporting programs for postpartum women, as they tend to be costly, and are not covered by national health insurance. To date, no central government agency has implemented a comprehensive KM management program for postpartum women. However, as part of a public health care project the Korean Medicine-Based Postnatal Healthcare Program (KMPHP) was set up by the National Medical Center (NMC), and has operated since 2017. Moreover, it has expanded the range of eligible participants for the KMPHP to focus mothers residing in Seoul (Type 1 or 2 medical aid beneficiaries or national health insurance subscribers with a median income of ≤ 80%), who have given birth in the last three months. The reason for the KMPHP is to prevent or treat postnatal symptoms, physical and emotional discomfort, and to aid rapid postpartum recovery.
- All public health projects need to measure the direction and magnitude of benefits and harm by conducting robust evaluation studies. This study aimed to quantitatively evaluate the effectiveness and safety of the KMPHP run by the NMC with the help of an adjusted before-and-after comparative study design using data obtained from mothers who participated in the KMPHP.
Introduction
- This was a performance evaluation study in which a public hospital conducted public health projects targeting the vulnerable and evaluated the effectiveness of the projects. As this study was aimed at all mothers who participated in the KMPHP, a target sample size to power the study was not calculated; the medical records of all postpartum women enrolled in the KMPHP were retrospectively analyzed.
- The study protocol was approved by the Institutional Review Board of the NMC (IRB no.: NMC-2006-019) on June 11, 2020. Informed consent was waived by the IRB because this was a retrospective study.
- 1. Participants of the KMPHP
- This retrospective study included postpartum women who had given informed consent to participate in the KMPHP, after reading posters or pamphlets about the program placed within hospitals, or after being informed about it at a health center between April 1, 2019 and April 30, 2020. All participants in the KMPHP who had completed the postpartum symptoms questionnaire before and after participation in the program, and for whom outcome variables of interest could be assessed, were included in this study. In contrast, postpartum women who had visited a hospital for Sanhupung, but were not eligible to participate in the KMPHP, or whose postpartum symptoms questionnaire results were not obtained, were excluded from the study.
- 2. The KMPHP
- During their 1st visit, mothers had received an in-person consultation and examination from a KMD and had been prescribed HM for postpartum recovery based on their symptoms and body constitution. They were prescribed a 20-day supply of HM to be taken twice daily. Additional HMs had also been prescribed depending on the conditions of the participants of the KMPHP.
- If necessary, an experienced KMD with more than 10 years of clinical experience performed acupuncture, electroacupuncture, pharmacoacupuncture, Chuna manual therapy (CMT), and dry cupping based on chief complaints. Non-pharmacological treatments, including acupuncture and CMT, had been scheduled according to the mothers’ convenience.
- 3. Outcome measurements
- Three outcomes including quality of life (QoL), pain intensity, and postpartum depression levels were assessed. QoL was measured using the EuroQol-5 Dimension-5L (EQ-5D-5L) and EuroQol Visual Analog Scale (EQ-VAS); pain intensity and depression were measured using the Numeric Rating Scale (NRS) and the Korean Version of the Edinburgh Postnatal Depression Scale (K-EPDS), respectively [9–11].
- The EQ-5D-5L is a QoL measurement tool consisting of five areas: mobility, self-care, manual activities, pain/discomfort, and anxiety/depression. There are five domains for each area, and it is reported that the ceiling effect is less and validity is higher than EQ-5D-3L. The Korean version of this tool was developed, and the validity and reliability were checked [9]. The EQ-VAS is a scale that measures QoL in terms of state of health and it does so in the form of self-reporting using an analogue vertical line from 0 (the worst) to 100 (the best), and is an auxiliary measure for the EQ-5D. The NRS is a method of determining pain by expressing the degree of pain one is currently feeling in the range of 0 (no pain) to 10 (extreme pain), and can be evaluated very simply and quickly [10]. The EPDS consists of 10 questions that indicate the emotional state of the mother in the past week, including depression, anxiety and fear, guilt, and self-harm accidents. For each question, 0,1,2, or 3 points are given according to the symptoms, and the total score of the 10 questions is between 0 and 30; the higher the score, the higher the risk of postpartum depression. In this study, the K-EPDS, which reported adequate validity and reliability, was used [11].
- Outcome variables were measured once at the first visit and again after a maximum of two herbal prescriptions were completed.
- Based on the examination records from the first outpatient visit, the following general characteristics of the mothers were analyzed: age, body mass index (BMI), history of alcohol use, smoking status, and pregnancy and delivery-related characteristics. For the characteristics related to postpartum symptoms, the chief complaints and accompanying symptoms were investigated using a questionnaire.
- 4. Statistical analysis
- Continuous variables were expressed as mean ± standard deviation or median and interquartile range depending on the normality, and categorical variables were expressed as count and percentage (n, %) with the results of the Chi-square test Either A paired t test or paired-sample Wilcoxon test, followed by a Shapiro-Wilks normality test was used to compare outcome variables before and after treatment.
- In addition, to precisely analyze the effectiveness of each component of the program such as HM and non-pharmacological KM interventions, cross-sectional, time series, feasible generalized and least squares method (FGLS) regression analysis was used. FGLS has advantages in adjusting confounding factors, heteroscedasticity, and autocorrelation due to repeated measurements. The effect of each treatment was identified through the main explanatory variables like the number of HM prescriptions and whether or not non-pharmacological treatments were used, and synergistic effects were confirmed through the 3-way interaction term of the two variables and pre-post variable.
- All statistical analyses were performed using STATA MP Version 16.1 (Strata Corp, College Station, TX, USA) with the level of statistical significance at p < 0.05.
Material and Methods
- 1. General characteristics of patients
- A total of 37 postpartum mothers had completed the postpartum symptoms questionnaire before and after participating in the KMPHP. The mean age range of the women was 28–43 years, they were normal to overweight, and most women had previously more than 1 child. Most women chose to give birth naturally and breast fed their child. Postpartum care was mostly late for these women (Table 1).
- 2. Characteristics and treatment of postpartum symptoms
- The most common complaint was joint pain (81.09%). Other symptoms included cold sensation, swelling, dizziness, lower abdominal pain, and dyspepsia (Supplementary Table 1).
- The most common accompanying symptom was joint pain (n = 37, 100%), followed by digestive discomfort (n = 13, 35.14%), cold sensation (n = 9, 24.33%), defecation discomfort (n = 6, 16.22%), and swelling (n = 4, 10.81%; Supplementary Table 1).
- All 37 mothers were prescribed HM based on their symptoms (n = 37, 100%; Supplementary Table 2). The second most common intervention was acupuncture (n = 27, 72.97%) and the third was dry cupping (n = 22, 59.46%; Supplementary Table 2).
- 3. Program evaluation
- After completing the KMPHP, changes in the outcome variables K-EPDS, EQ-5D-5L, EQ-VAS, and NRS scores were analyzed using a paired-sample Wilcoxon test, as the normal distribution was not assumed by the Shapiro-Wilks normality test. The mean number of days until the measurement of outcome variables was 36.30 ± 12.75 days after the first visit.
- The mean K-EPDS score significantly decreased from 8 (4–9) before treatment to 5 (2–9) after treatment (p < 0.01). The mean EQ-5D-5L score significantly increased from 0.82 (0.78–0.82) before treatment to 0.83 0.81–0.86) after treatment (p = 0.02). The mean EQ-VAS score, a QoL indicator, significantly increased from 70 (60–80) before treatment to 80 (70–85) after treatment (p < 0.01). The mean NRS score, a subjective pain measure, decreased from 4 (3–6) to 3 (2–3); however, the difference was not significant (p = 0.05; Table 2).
- KM doctors in the KMPHP provided individualized treatment for the participants based on the original KM diagnosis, and they were delivered by KM modalities (Supplementary Table 2). At this time, in order to precisely analyze the effect of each KM intervention on the outcomes, FGLS regression analysis with confounding factors adjusted, was conducted.
- The K-EPDS assesses postpartum mothers’ emotional states. Relatively the older mothers were, the higher the scores for depression were(p < 0.001). And mothers who had undergone a Cesarean section scored higher than those who had given birth through vaginal delivery (p < 0.001). As a result of analyzing the effects of HM and non-pharmacological intervention through interaction terms, HM decreased the EPDS scores 3.36 (p < 0.001). Mothers who had undergone non-pharmacological treatments, including acupuncture, dry cupping, pharmacoacupuncture and CMT with additional HM prescription showed a significant EPDS score reduction of −3.89 (p < 0.001; Table 2).
- The EQ-5D-5L measures QoL. The mean EQ-5D-5L scores were significantly lower among older mothers, those with a history of alcohol use and multipara, and those who had undergone a Cesarean section, whereas scores were significantly higher among breastfeeding mothers (p < 0.001). HM significantly increased the mean EQ-5D-5L score by 0.07 when the effects of other explanatory variables were controlled (p < 0.001). Mothers who received NP treatment plus additional HM had a significantly lower QoL from the beginning (p < 0.001) and showed relatively less improvement after treatment compared with mothers who took HM only once (p < 0.001).
- Older mothers, and those with a history of alcohol use, high BMI, and multipara had significantly lower EQ-VAS scores (p < 0.001). Mothers who had undergone a Cesarean section and those who were breastfeeding had significantly higher EQ-VAS scores (p < 0.001). HM significantly improve the EQ-VAS score by 12.35 (p < 0.001), indicating an improvement in QoL. Adding non-pharmacological treatment significantly increased the EQ-VAS score to 4.14 (p < 0.001). In addition, a synergistic additive effect of an improvement of 8.21 was reported when additional HM was administered (p < 0.001).
- The NRS is a subjective measure of pain. NRS score significantly decreased with lower maternal age (p < 0.001), but significantly increased with a history of using alcohol, and higher BMI (p < 0.001). Similarly, multiparous mothers (p < 0.001) had significantly higher NRS scores. HM significantly reduced the mean NRS score by −2.03 (p < 0.001). The mean NRS score for mothers who received both HM and non-pharmacological treatment additionally decreased to −0.96 (p = 0.03), but no significant difference was observed among mothers who received HM for a longer period of time (p = 0.41; Table 3).
- One participant in the KMPHP had diarrhea during the first three days of taking her medications. None of the women reported unusual responses from their children, and 14 women reported that their children had healthy growth. Some women reported that the hands and feet of their children got warmer after breastfeeding.
Results
2.1. Chief concerns
2.2. Accompanying symptoms
2.3. Treatment intervention
3.1. Pre- and post-program evaluation
3.2. Evaluation of the effect of each intervention on outcomes using FGLS
3.3. Adverse drug reactions and infant’s response
- The need for postpartum medical interventions and management is being emphasized with the increasing number of pregnant mothers of advanced maternal age (≥ 35 years), high risk pregnancies, multiple pregnancies due to assisted reproductive technology, and child delivery by Cesarean section [12]. Statistics from Korean National Health Insurance during 2008 to 2012 on pregnancy and postpartum conditions/diseases, revealed the number of patients increased by 7.9% per year, from approximately 53,000 in 2008, to 67,000 in 2012. This increase was substantial considering the decreasing trend in the number of births. Similarly, medical costs increased at an annual rate of 9.9% [13].
- Over the last decade, complementary and alternative medicine (CAM) has been used worldwide for maternity management and for patients with chronic conditions/diseases [14,15]. Women from Asian and Latin cultural backgrounds prefer using specific conventions based on CAM theory [16,17]. A Chinese study reported that 45% of mothers take HMs after childbirth and undergo CAM treatments, including acupressure, massage, reflexology, and acupuncture, combined with HM [18,19]. Some studies have reported significant improvement among mothers with postpartum depression after HM interventions, electroacupuncture, and moxibustion [20].
- KM has the original concept of Sanhupung, which covers various symptoms and weaknesses experienced by postpartum mothers. Korean mothers, particularly those with high-risk pregnancies, are deeply concerned about this [21]. As it is known that Sanhupung can be effectively prevented and treated with KM, and the NMC of Korea has recently (2017) implemented a public health program that provides such treatments to vulnerable mothers [22].
- The total number of women studied in this retrospective evaluation analysis was 37, with the mean age being 34.84 ± 2.81 years. The most common postpartum symptom of Sanhupung was joint pain (81.09%), followed by cold sensation and swelling, which is consistent with the findings by Jang et al [23]. A study in China, which has a similar postpartum management culture, reported the main purpose of postpartum CAM was to reduce postpartum pain (22.20%) and give relief to the mothers [19]. The high percentage of patients with postpartum joint pain may be attributed to the physiological changes that occur during pregnancy due to secretion of the hormone relaxin (which relaxes the ligaments in the pelvis), and the higher preference for KM treatments for musculoskeletal conditions/diseases.
- All participants of the KMPHP had received a personalized prescription from the KMD for HM and additional non-pharmacological treatments depending on their symptoms and situations. In this study, HM, including Xiong qui tiao xue yin, Gui zhi tang, Da bu tang, and Bu xu tang, was commonly prescribed (Supplementary data). Acupuncture was the most common non-pharmacological treatment (n = 27, 72.97%), followed by dry cupping (n = 22, 29.73%). Ten women (27.03%) had received pharmacoacupuncture. No HM-associated adverse drug reactions were observed in this study. A previous study examining the effects of HM among 498 postpartum mothers also reported no adverse drug reactions, indicating that postpartum use of HM is relatively safe [24].
- In the paired-sample Wilcoxon test assessment of the KMPHP’s effectiveness, significant improvements in the K-EPDS, EQ-5D-5L, and EQ-VAS scores were observed upon program completion (p < 0.01, p = 0.02, p < 0.01, respectively). Of the 37 women, 20 (54.05%) showed an improvement in NRS score by a value of at least 1. The minimal clinically important difference (MCID) for the EPDS has been seldom explored, and there is no consensus about how to determine the optimal MCID value. A recent study recommended an improvement of 4 points, but the study was conducted on participants in the KMPHP with postpartum depression; in this current study, most mothers had Sanhupung, which consisted of mainly physical symptoms, so there was little room for improvement after treatment. Thus, it was unlikely to reach MCID [25]. The EQ-5D-5L significantly improved by 0.01 and mean EQ-VAS score significantly increased from 70 before the program to 80 (p < 0.01) after the program. However, no identifiable single MCID for the EQ-5D values or EQ-VAS scores was found; the estimates varied based on patient group, clinical context, and sociodemographic factors [26]. Furthermore, there is currently no agreement on the MCID in pain and little is known about which contextual factors cause variation [27]. In this current study, the improvement of the NRS score was not statistically significant and could not be more than the MCID. However, a previous qualitative study reported the benefits of pain reduction and improved psychological health through the KMPHP [28]. Although not known by quantitatively measured values, this qualitative study showed the value of the program, which could not be known simply through objective evaluation indicators via patients’ narratives.
- A FGLS regression analysis was performed to assess the effects of the KMPHP by intervention while controlling for the effects of other explanatory variables. HM significantly decreased the K-EPDS scores by −3.36 (p < 0.001) and adding both non-pharmacological treatment and a 2nd HM prescription significantly reduced the mean K-EPDS score by −3.89 (p < 0.001). This indicated that greater alleviation of postpartum depression may be achieved using non-pharmacological treatments such as acupuncture, pharmacoacupuncture, and CMT combined with HM. Acupuncture, one of non-pharmacological interventions of KM, may relieve depression and anxiety in infertile women and shows similar therapeutic effects to antidepressants but with fewer side effects [29,30]. It has also been reported that KM-based treatment of postpartum depression, such as acupuncture, is more effective and causes fewer side effects compared with antidepressant monotherapy [31]. Consultation experience and establishing positive relationships between the KMD and participants in the KMPHP during non-pharmacological treatment has also been reported to enhance the effect of the treatment [32].
- In Western medicine, treatment of postpartum depression is classified into pharmacological treatment based on antidepressants and non-pharmacological treatment, including cognitive behavioral therapy. However, many postpartum women reject Western medication for reasons related to breastfeeding and drug side effects [33]. Based on these results, HM from natural products and non-pharmacological treatments of KM can be considered as an alternative treatment for postpartum depression.
- HM significantly improved the mothers’ QoL score on the EQ-5D-5L by 0.07 (p < 0.01) and the EQ-VAS by 12.35 (p < 0.001), while the effects of other confounding variables were controlled. In contrast, the effects of non-pharmacological treatment and additional HM treatment on maternal QoL were inconsistent in both parameters. As healthcare services are becoming more patient-oriented, understanding patient-reported outcomes such as QoL is becoming increasingly important. Assessing the patients!/subjective experience is essential while making clinical decisions or policies. Thus, the observation wherein HM-based interventions significantly improved the mothers!/QoL is meaningful.
- NRS scores decreased significantly with increasing age and was significantly higher among those with a greater BMI. Similarly, the scores were significantly high among multiparous mothers and those who had a history of alcohol consumption. The mean NRS score significantly decreased by −2.03 among mothers who had received HM (p < 0.001). Mothers who had undergone additional non-pharmacological treatments achieved a synergistic significant NRS score reduction of −0.96 compared with those who did not (p = 0.03). Acupuncture widely alleviates neuroinflammation and effectively reduces pain by reducing prostaglandin-endoperoxide synthase 2 levels or inducing the secretion of analgesic substances, and by inhibiting intrinsic pain via diffuse noxious inhibitory control [34]. The current study results suggest that HM may similarly manage postpartum pain effectively.
- Analgesics are used to treat postpartum pain in Western medicine, especially for postpartum joint pain [35]. Analgesics may pass into breast milk but not at doses likely to cause hepatotoxicity. However, alternative treatments may be suitable substitutes for analgesics if there is concern [36]. The postpartum health management program assessed in this study demonstrated that various KM-based interventions, such as HM, acupuncture, pharmacoacupuncture, and CMT, effectively manage postpartum symptoms.
- A limitation of this study was that the association between each reported symptom and the specific intervention could not be fully examined due to the small sample size. The study outcome could be affected by the complex treatments used for different patients and various complaints. The comorbidity of patients and evaluation results for infants were not reported. Furthermore, the number of treatment sessions, such as acupuncture and CMT, were limited as it was difficult for postpartum mothers to visit hospitals. In addition, as this program was executed by a public medical institution with a public medical budget, there was a limit to supporting medical cost per person. As this study was conducted retrospectively, a control group could not be included. In the future, a follow-up study examining the long-term effects of the KMPHP in a larger number of mothers or comparing outcome variables with control groups at different time points is needed.
Discussion
- The KMPHP comprising pharmacological and non-pharmacological treatments showed significant effects on postpartum depression, QoL, and levels of pain. Significant synergistic effects between HM and non-pharmacological treatments were observed using the K-EPDS, EQ-VAS and NRS scores. This study exploratively showed that the KMPHP could potentially effectively alleviate pain and depression, as well as improve QoL although a larger sample size in a controlled study is necessary.
Conclusion
Supplementary Materials
-
Author Contributions
Conceptualization: JS. Methodology: JL and MP. Formal analysis: MP. Data curation: DL and HP. Writing–original draft preparation: JS. Writing–review and editing: HP, IY and MP. Visualization: DL. Supervision: JL and MP. All authors have read and agreed to the published version of the manuscript.
-
Conflicts of Interest
The authors declare that there is no conflict of interest.
-
Ethical Statement
This study was approved by the Institutional Review Board of the National Medical Center, Seoul, Korea (no.: NMC-2006-019). The requirement for informed consent was waived owing to the retrospective nature of the study.
-
Funding
This work was supported by the National Medical Center, Republic of Korea (grant no.: NMC 2020-PR-02).
-
Date Availability
All relevant data are included in this manuscript.
Article information
| Variables | Frequency (%)/mean ± SD (range) | ||
|---|---|---|---|
| Age (y) | 34.84 ± 2.81 (28–43) | ||
|
|
|||
| History of alcohol use | No | 27 | (72.97) |
| Yes | 10 | (27.03) | |
|
|
|||
| BMI | 23.76 ± 3.45 (17.63–32.91) | ||
|
|
|||
| Obstetrics history | Primipara | 15 | (40.54) |
| Multipara | 22 | (59.46) | |
|
|
|||
| Delivery method | Natural | 25 | (67.57) |
| Cesarean | 12 | (32.43) | |
|
|
|||
| Feeding | Bottle/mixed | 17 | (45.95) |
| Breast-feeding | 20 | (54.05) | |
|
|
|||
| Start of postpartum period care* | Early | 12 | (32.43) |
| Late | 25 | (67.57) | |
| Rating scale/questionnaire | Score before treatment (median, IQR) | Score after treatment (median, IQR) | p* |
|---|---|---|---|
| K-EPDS | 8 (4–9) | 5 (2–9) | < 0.001† |
| EQ-5D-5L | 0.82 (0.78–0.82) | 0.83 (0.81–0.86) | 0.02†† |
| EQ-VAS | 70 (60–80) | 80 (70–85) | < 0.001†† |
| NRS | 4 (3–6) | 3 (2–3) | 0.05 |
* K-EPDS, EQ-5D-5L, EQ-VAS, NRS scores are assumed to be non-normally distributed based on the Shapiro-Wilks normality test.
† Statistically significantly decreased from baseline (p using paired-sample Wilcoxon test).
†† Statistically significantly increased from baseline (p using paired-sample Wilcoxon test).
EQ-5D-5L = EuroQol-5 dimension-5L; EQ-VAS = EuroQol visual analogue scale; K-EPDS = Korean version of Edinburgh postnatal depression scale; NRS = numeric rating scale.
| Variables | K-EPDS | EQ-5D-5L | EQ-VAS | NRS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|||||||||
| Coef. | Std. error | p > z | Coef. | Std. error. | p > z | Coef. | Std. error. | p > z | Coef. | Std. error. | p > z | |
| Age | 0.20* | 0.02 | 0.00 | −0.00* | 0.00 | 0.00 | −0.39* | 0.12 | 0.00 | −0.32* | 0.02 | 0.00 |
|
|
||||||||||||
|
Alcohol history (ref. no) Yes |
0.36 | 0.24 | 0.13 | −0.02* | 0.00 | 0.00 | −14.18* | 0.70 | 0.00 | 0.53* | 0.19 | 0.01 |
|
|
||||||||||||
| BMI | 0.02 | 0.03 | 0.56 | 0.01* | 0.00 | 0.00 | −0.38* | 0.05 | 0.00 | 0.20* | 0.03 | 0.00 |
|
|
||||||||||||
|
Obstetric history (ref. primipara) Multipara |
−0.35 | 0.23 | 0.13 | −0.01* | 0.00 | 0.00 | −11.21* | 0.58 | 0.00 | 0.58* | 0.16 | 0.00 |
|
|
||||||||||||
|
Delivery method (ref. natural) Cesarean |
0.22* | 0.03 | 0.00 | −0.00 | 0.00 | 0.31 | 5.91* | 0.78 | 0.00 | 0.47 | 0.26 | 0.07 |
|
|
||||||||||||
|
Feeding (ref. bottle/mixed) Breastfeeding |
−0.40 | 0.25 | 0.11 | 0.01* | 0.00 | 0.00 | 2.66* | 0.76 | 0.00 | 0.05 | 0.24 | 0.19 |
|
|
||||||||||||
|
Postpartum period (ref. no) Yes |
0.38 | 0.26 | 0.14 | −0.00 | 0.00 | 0.68 | −0.39 | 0.50 | 0.43 | −0.32 | 0.18 | 0.08 |
|
|
||||||||||||
| POST# NP # HM‡ | ||||||||||||
|
|
||||||||||||
| 0 0 1 (ref.) | ||||||||||||
|
|
||||||||||||
| 0 1 1 | 0.32 | 0.53 | 0.55 | −0.02* | 0.00 | 0.00 | 0.01 | 0.73 | 0.99 | −0.51 | 0.30 | 0.09 |
|
|
||||||||||||
| 0 1 2 | −2.53* | 0.41 | 0.00 | −0.06* | 0.00 | 0.00 | 5.16* | 0.75 | 0.00 | 0.18 | 0.22 | 0.41 |
|
|
||||||||||||
| 1 0 1 | −3.36* | 0.24 | 0.00 | 0.07* | 0.00 | 0.00 | 12.35* | 1.93 | 0.00 | −2.03* | 0.43 | 0.00 |
|
|
||||||||||||
| 1 1 1 | −1.94 | 0.55 | 0.73 | −0.01* | 0.00 | 0.03 | 4.14* | 0.80 | 0.00 | −0.96* | 0.44 | 0.03 |
|
|
||||||||||||
| 1 1 2 | −3.89* | 0.62 | 0.00 | −0.04* | 0.01 | 0.00 | 8.21* | 1.48 | 0.00 | 0.18 | 0.22 | 0.41 |
|
|
||||||||||||
| cons | 1.14* | 0.01 | 0.00 | 97.63* | 3.23 | 0.00 | 10.24* | 0.76 | 0.00 | |||
| Wald χ2 (12) = 2.58e+10 | Wald χ2 (12) = 64,908.31 | Wald χ2 (12) = 12,205.22 | Wald χ2 (12) = 15,271.84 | |||||||||
| prob > χ2 = 0.00 | prob > χ2 = 0.00 | Prob > χ2 = 0.00 | prob > χ2 = 0.00 | |||||||||
* Statistically significant (p < 0.05).
† Cross-sectional, time-series, feasible, generalized least squares (FGLS) regression.
‡ POST: dummy variable indicating pre- or post-intervention (0 or 1).
# Interaction.
HM: the number of herbal medicine prescription (1 or 2).
NP: whether the non-pharmacological treatments were provided or not (0 or 1).
note: 0./1. Post # 0.NP # 2.HM identifies no observations in the sample.
BMI = body mass index; EQ-5D-5L = EuroQol-5 dimension-5L; EQ-VAS = EuroQol visual analogue scale; HM = herbal medicine; K-EPDS = Korean version of Edinburgh postnatal depression scale; NRS = numeric rating scale; NP = non-pharmacological intervention.
- [1] Li W, Yin P, Lao L, Xu S. Effectiveness of acupuncture used for the management of postpartum depression: a systematic review and meta-analysis. BioMed Res Int 2019;2019:6597503. ArticlePubMedPMCPDF
- [2] Strelow B, Fellows N, Fink SR, O’Laughlin DJ, Radke G, Stevens J, et al. Postpartum depression in older women. JAAPA 2018;31(3):15−8.Article
- [3] The Society of Korean Medicine Obstetrics and Gynecology. Oriental obstetrics & gynecology. Seoul (Korea), Euiseongdang, 2012, [in Korean].
- [4] Hodgkinson EL, Smith DM, Wittkowski A. Women’s experiences of their pregnancy and postpartum body image: a systematic review and meta-synthesis. BMC Pregnancy Childbirth 2014;14:330. ArticlePubMedPMCPDF
- [5] Oh SK, Noh EJ, Choi SJ, Kim DI. A study for the establishment of the diagnostic definition of Sanhupung (U32.7) using the Delphi method. J Korean Obstet Gynecol 2021;34(2):16−30. [in Korean] https://koreascience.kr/article/JAKO202116954659802.page.
- [6] Withers M, Kharazmi N, Lim E. Traditional beliefs and practices in pregnancy, childbirth and postpartum: a review of the evidence from Asian countries. Midwifery 2018;56:158−70.ArticlePubMed
- [7] Hwang HJ, Kim DC. The clinical analysis of Sanhupung patients and treatment at an Oriental medicine hospital. J Korean Obstet Gynecol 2020;33(4):56−74. [in Korean] https://koreascience.kr/article/JAKO202033759656032.page.
- [8] MacArthur C. What does postnatal care do for women’s health? Lancet 1999;353(9150):343−4.ArticlePubMed
- [9] Kim SH, Ahn J, Ock M, Shin S, Park J, Luo N, et al. The EQ-5D-5L valuation study in Korea. Qual Life Res 2016;25(7):1845−52.ArticlePubMedPDF
- [10] Thong ISK, Jensen MP, Miró J, Tan G. The validity of pain intensity measures: what do the NRS, VAS, VRS, and FPS-R measure? Scand J Pain 2018;18(1):99−107.ArticlePubMed
- [11] Kim YK, Won SD, Lim HJ, Choi SH, Lee SM, Shin YC, et al. Validation study of the Korean version of Edinburgh Postnatal Depression Scale (K-EPDS). Mood Emot 2005;3(1):42−9. http://www.moodandemotion.org/journal/view.html?uid=285&vmd=Full.
- [12] Youn JH, Jeong IS. Predictors of postpartum depression: prospective cohort study. J Korean Acad Nurs 2013;43(2):225−35.ArticlePubMed
- [13] Kim PW, Kim AN, Jang HC, Lee EH. A prospective observational study on symptoms of the postpartum women with Korean medicine treatment during six weeks after childbirth. J Korean Obstet Gynecol 2017;30(4):114−34. [in Korean] https://kiss.kstudy.com/Detail/Ar?key=3564240.
- [14] Yeam CT, Yo TE, Tan YLC, Liew A, Seng JJB. Complementary and alternative medicine therapies for uremic pruritus-A systematic review of randomized controlled trials. Complement Ther Med 2021;56:102609. ArticlePubMed
- [15] Chu SWF, Yeam CT, Low LL, Tay WY, Foo WYM, Seng JJB. The role of mind-body interventions in pre-dialysis chronic kidney disease and dialysis patients - A systematic review of literature. Complement Ther Med 2021;57:102652. ArticlePubMed
- [16] Hung P. Traditional Chinese customs and practices for the postnatal care of Chinese mothers. Complement Ther Nurs Midwifery 2001;7(4):202−6.ArticlePubMed
- [17] Kim-Godwin YS. Postpartum beliefs and practices among non-Western cultures. MCN Am J Matern Child Nurs 2003;28(2):74−8. quiz 79-80.ArticlePubMed
- [18] Tang L, Lee AH, Binns CW, Hui YV, Yau KKW. Consumption of Chinese herbal medicines during pregnancy and postpartum: a prospective cohort study in China. Midwifery 2016;34:205−10.ArticlePubMed
- [19] Zeng Y, Zhou Y, Chen P, Luo T, Huang M. Use of complementary and alternative medicine across the childbirth spectrum in China. Complement Ther Med 2014;22(6):1047−52.ArticlePubMed
- [20] Deligiannidis KM, Freeman MP. Complementary and alternative medicine therapies for perinatal depression. Best Pract Res Clin Obstet Gynaecol 2014;28(1):85−95.ArticlePubMedPMC
- [21] Bae GM, Lee IS. The study to investigate the recognition on postpartum symptom among Korean, Korean resident in America and American. J Korean Obstet Gynecol 2010;23(2):131−44. [in Korean] http://www.koreascience.or.kr/article/JAKO201021147396074.j.
- [22] Bak JY, Park JK, Park KY, Kim TH. A study about the satisfaction of Oriental medical postpartum care. J Korean Obstet Gynecol 2009;22(4):173−86. [in Korean] https://oobgy.jams.or.kr/po/volisse/sjPubsArtiPopView.kci?soceId=INS000001864&artiId=SJ0000000644&sereId=SER000000001&submCnt=1&indexNo=14.
- [23] Jang SR, Park YS, Kim DC. The clinical analysis of 104 Sanhupung patients that visited at an Oriental medicine hospital. J Korean Obstet Gynecol 2010;23(3):192−204. [in Korean] https://oobgy.jams.or.kr/po/volisse/sjPubsArtiPopView.kci?soceId=INS000001864&artiId=SJ0000000686&sereId=SER000000001&submCnt=1&indexNo=15.
- [24] Kim PW, Jung SY, Lee EH. An analysis of domestic researches on the prescriptions of Korean herbal medicine used during postpartum period. J Korean Obstet Gynecol 2018;31(4):128−46. https://oobgy.jams.or.kr/po/volisse/sjPubsArtiPopView.kci?soceId=INS000001864&artiId=SJ0000001139&sereId=SER000000001&submCnt=5&indexNo=8.
- [25] Mao F, Sun Y, Wang J, Huang Y, Lu Y, Cao F. Sensitivity to change and minimal clinically important difference of Edinburgh postnatal depression scale. Asian J Psychiatr 2021;66:102873. ArticlePubMed
- [26] Devlin N, Parkin D, Janssen B. Advanced Topics. Methods for Analysing and Reporting EQ-5D Data. Cham (Switzerland), Springer, 2020.Article
- [27] Olsen MF, Bjerre E, Hansen MD, Tendal B, Hilden J, Hróbjartsson A. Minimum clinically important differences in chronic pain vary considerably by baseline pain and methodological factors: systematic review of empirical studies. J Clin Epidemiol 2018;101:87−106e2.ArticlePubMed
- [28] Lee DE, Suh HW, Park HS, Youn I, Park M, Seo J. Mothers’ Experiences of Childbirth and Perspectives on Korean Medicine-Based Postpartum Care in Korea: A Qualitative Study. Int J Environ Res Public Health 2022;19(9):5332. ArticlePubMedPMC
- [29] Isoyama D, Cordts EB, de Souza van Niewegen AM, et al. Effect of acupuncture on symptoms of anxiety in women undergoing in vitro fertilisation: a prospective randomised controlled study. Acupunct Med 2012;30(2):85−8.ArticlePubMedPDF
- [30] Gartlehner G, Gaynes BN, Amick HR, Asher GN, Morgan LC, Coker-Schwimmer E, et al. Comparative benefits and harms of antidepressant, psychological, complementary, and exercise treatments for major depression: an evidence report for a clinical practice guideline from the American College of Physicians. Ann Intern Med 2016;164(5):331−41.ArticlePubMed
- [31] Li M, Niu J, Yan P, Yao L, He W, Wang M, et al. The effectiveness and safety of acupuncture for depression: an overview of meta-analyses. Complement Ther Med 2020;50:102202. ArticlePubMed
- [32] MacPherson H, Mercer SW, Scullion T, Thomas KJ. Empathy, enablement, and outcome: an exploratory study on acupuncture patients’ perceptions. J Altern Complement Med 2003;9(6):869−76.ArticlePubMed
- [33] Pearlstein T, Howard M, Salisbury A, Zlotnick C. Postpartum depression. Am J Obstet Gynecol 2009;200(4):357−64.ArticlePubMedPMC
- [34] Li K, Giustini D, Seely D. A systematic review of acupuncture for chemotherapy-induced peripheral neuropathy. Curr Oncol 2019;26(2):e147−54.ArticlePubMedPMCPDF
- [35] East CE, Sherburn M, Nagle C, Said J, Forster D. Perineal pain following childbirth: prevalence, effects on postnatal recovery and analgesia usage. Midwifery 2012;28(1):93−7.ArticlePubMed
- [36] Simbar M, Shadipour M, Salamzadeh J, Ramezani-Tehrani F, Nasiri N. The combination of “Pimpinella anisum, Apium graveolens and Crocus sativus (PAC)” is more effective than “mefenamic acid” on postpartum after-pain. J Herb Med 2015;5(1):20−5.Article
References
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite