Articles
- Page Path
- HOME > Perspect Integr Med > Volume 3(1); 2024 > Article
-
Review Article
A Modern Interpretation of Cold-Heat Pattern in Traditional Medicine with a Focus on Thermo-Regulation -
Younggwang Kim1
 , Jee Young Lee2, Joongho Lee3, Sanghun Lee1,3,*
, Jee Young Lee2, Joongho Lee3, Sanghun Lee1,3,* -
Perspectives on Integrative Medicine 2024;3(1):18-28.
DOI: https://doi.org/10.56986/pim.2024.02.003
Published online: February 22, 2024
1Department of Bioconvergence and Engineering, Graduate School, Dankook University, Yongin, Republic of Korea
2Integrative Cancer Center, Cha Ilsan Medical Center, Goyang, Republic of Korea
3BinaryTunerS Inc, Yongin, Republic of Korea
- *Corresponding author: Sanghun Lee, Department of Bioconvergence and Engineering, Graduate School, Dankook University, Yongin-si, Gyeonggi-do 16890, Republic of Korea, Email: shlee92@dankook.ac.kr
©2024 Jaseng Medical Foundation
This is an open access article under the CC BY-NC license (http://creativecommons.org/licenses/by-nc/4.0/).
- 445 Views
- 15 Download
Abstract
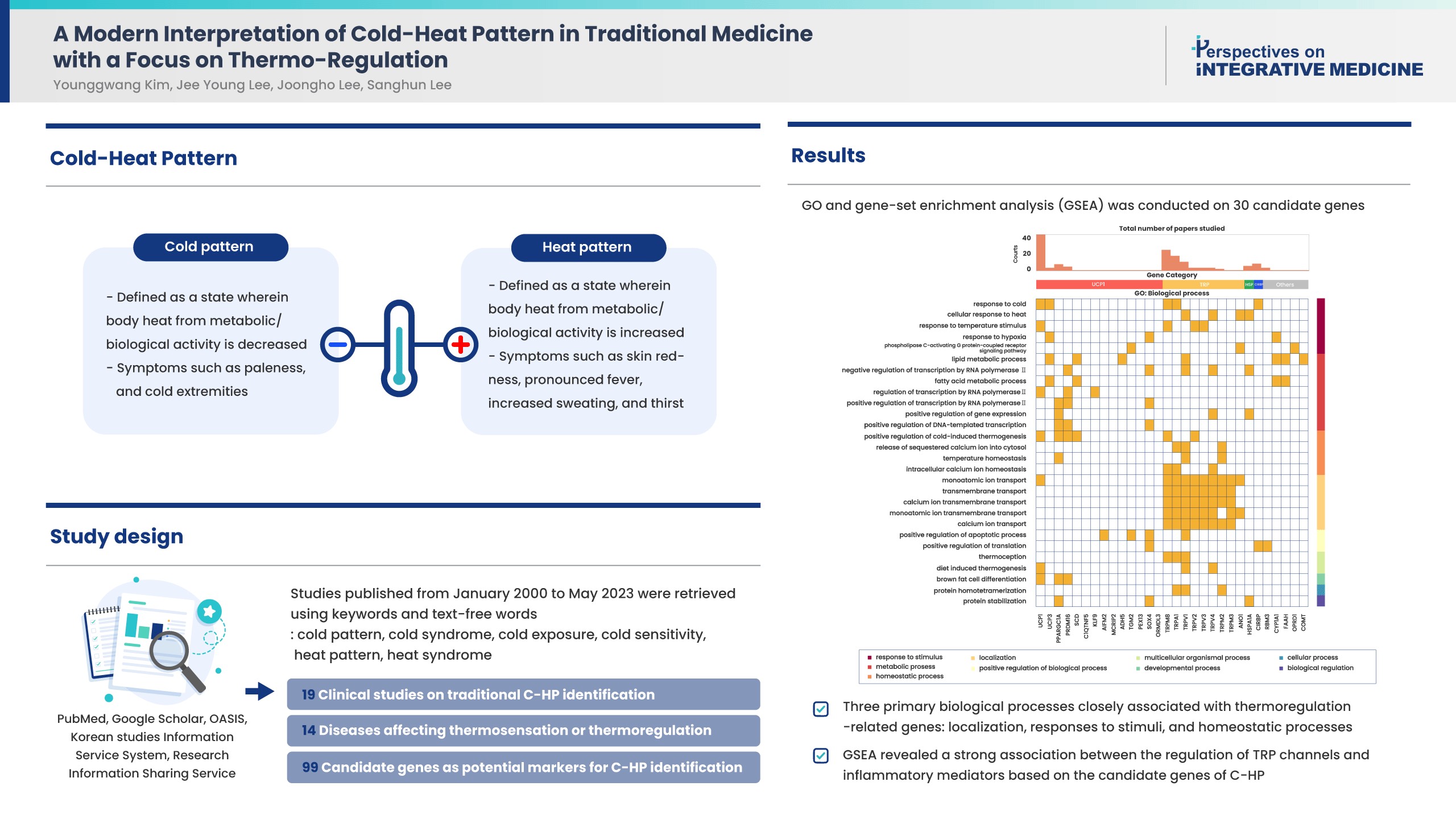
- Cold-heat patterns (C-HPs) in Traditional East Asian Medicine are essential for individually diagnosing and treating patients. However, the concept of C-HPs and their biological mechanisms (thermoregulation) remains unclear. C-HPs studies published between January 2000 and May 2023 were retrieved from 5 databases (PubMed, Google Scholar, OASIS, Korean studies Information Service System, and Research Information Sharing Service). Among the 8,373 articles screened, 132 were included in the review and categorized. Nineteen articles were clinical studies related to traditional concept of C-HP identification, 14 studies investigated diseases affecting thermosensation or thermoregulation, and 99 studies identified candidate genes as potential markers for C-HP identification. Further analysis, including gene ontology, and gene set enrichment analysis of the candidate genes, revealed 3 primary biological processes closely associated with thermoregulation-related genes, including localization, responses to stimuli, and homeostatic processes. Notably there was a significant association between the candidate genes and inflammatory mediator regulation of transient receptor potential channels (p < 0.001). A significant association between C-HPs and inflammation-related pathways across thermosensation-related and thermoregulation-related clinical and preclinical studies was observed, suggesting that the traditional concept of C-HPs should be studied further from an immunological perspective.
- In Traditional East Asian Medicine (TEAM), the concept of cold-heat patterns (C-HPs) refers to a specific diagnostic framework used to assess an imbalance in the Yin and Yang energies of the body, as well as the overall state of Qi (vital energy) and the blood [1]. The cold pattern is characterized by an excess of Yin energy or a deficiency of Yang energy in the body, whereas the heat pattern is characterized by an excess of Yang energy or a deficiency of Yin energy. A heat pattern is defined as a state wherein body heat from metabolic/biological activity is increased, whereas a cold pattern is defined as a state wherein these factors are decreased [2]. Individuals exhibiting a heat pattern might present with symptoms such as skin redness, pronounced fever, increased sweating, and thirst, whereas those with a cold pattern may display contrasting symptoms such as paleness, and cold extremities [3].
- Pattern identification and C-HPs in TEAM are essential for individual diagnosis and treatment of patients. Precision medicine currently follows the principles of pattern differentiation used in TEAM to provide personalized and customized care to patients [4,5]. However, the conventional C-HP is not clearly defined, and its unclear biological interpretation poses challenges in its application to precision medicine.
- Recent clinical studies on a wide range of diseases, including cancer and autoimmune diseases, have demonstrated the usefulness of C-HPs as prognostic or predictive markers in clinical practice [6,7]. Recent studies have incorporated more rigorous scientific methodologies to improve the validity of C-HPs. In particular, various omics technologies, including genomics, transcriptomics, proteomics, and metabolomics, have been used to gain a molecular-level understanding of C-HPs [8,9]. Recent twin studies have also supported a genetic influence on C-HPs, with C-HP heritability estimates of 33–40% in both sexes, irrespective of age [10]. However, this study was heterogeneous and focused exclusively on specific target diseases; furthermore, the potential generalizability of the C-HP concept and its biological mechanism (thermoregulation) remain unexplored.
- Here, a review was conducted of articles published since 2000 that investigated the concept of C-HP from 2 perspectives: (1) traditional concept of C-HPs in either clinical or preclinical settings; and (2) biological thermoregulation related to C-HPs.
- The objective of this review was to provide comprehensive insights into the molecular foundations of the traditional concept of C-HP diagnoses based on the biological aspects of C-HP.
Introduction
- 1. Search strategy
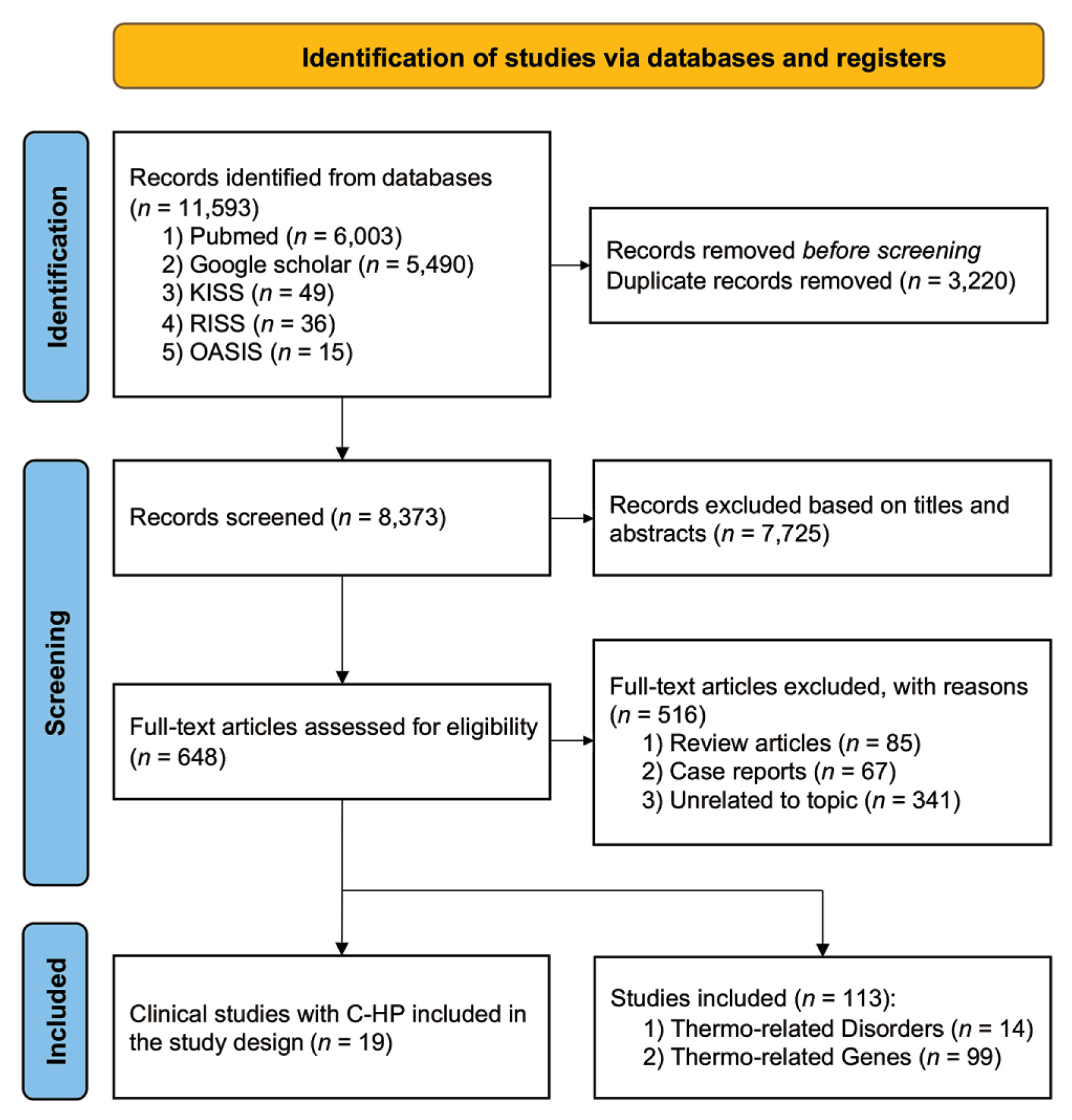
- All relevant studies were retrieved from 2 English (PubMed and Google Scholar) and 3 Korean databases (OASIS, Korean studies Information Service System, and Research Information Sharing Service). Studies published from January 2000 to May 2023 were retrieved using keywords and text-free words. The following words and terms were searched in article titles/abstracts: “cold pattern,” “cold syndrome,” “cold exposure,” “cold sensitivity,” “heat pattern,” and “heat syndrome.” These terms were translated into Korean when used to search the Korean databases. Relevant articles were manually screened to prevent omission of any research.
- 2. Selection criteria and quality assessment
- The article selection process aimed to identify all relevant studies that investigated either the traditional concept or the biological perspectives of C-HPs. The inclusion criteria were as follows: clinical studies related to traditional C-HP, research on thermoregulation-related disorders, C-HP-related omics studies, and studies on genes expressed in response to thermal stress.
- 3. Data extraction
- The results were processed using the reference management software EndNote (X9, Clarivate Analytics, London, United Kingdom) and duplicates were removed using “Find duplicates.” A total of 7,725 articles were excluded after screening the titles and abstracts. Two individuals manually screened and excluded articles based on the following criteria: full text not provided, review articles, case reports, and unrelated topics. Two independent reviewers undertook the study selection and quality assessments. This rigorous process ensured the credibility and validity of the included studies and their findings.
- 4. Gene ontology and Kyoto encyclopedia of genes and genomes pathway analysis
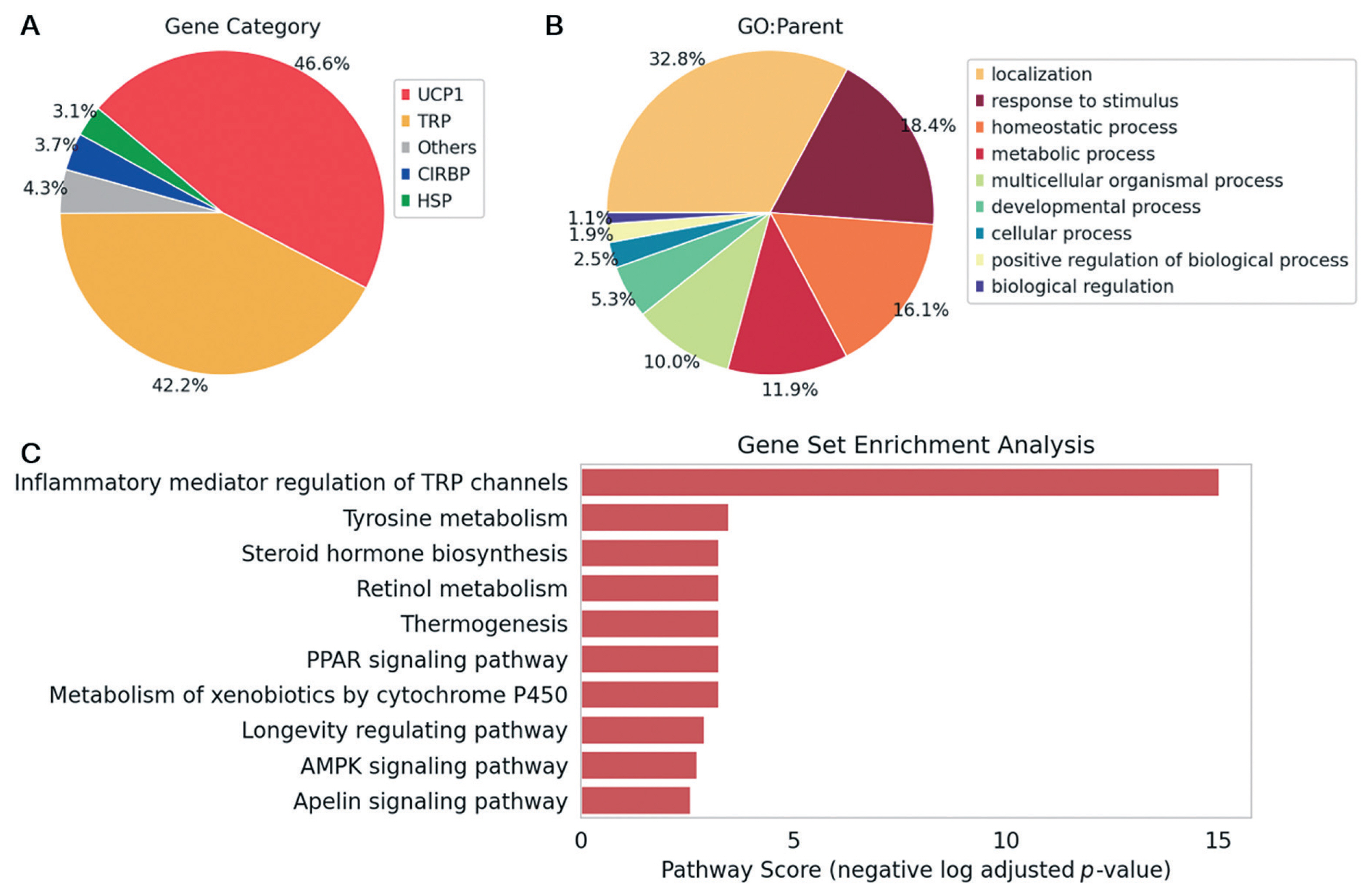
- Gene ontology (GO) annotations [11] were used to assess the biological mechanisms based on the gene list derived from our analysis which comprised 3 ontologies describing the biological processes, molecular functions, and cellular components of normal cells. To categorize genes based on their roles, the parent terms of each biological process was used. Furthermore, pathway analysis was performed by mapping the gene list to the Kyoto encyclopedia of genes and genomes database [12] using a comprehensive package for performing gene set enrichment analysis in Python (GSEApy) [13]. The adjusted p value was calculated using the Benjamini-Hochberg correction method and subsequently transformed using the negative logarithm for pathway score analysis.
Materials and Methods
- 1. Characteristics of the included studies
- A total of 132 articles were selected and further classified into 3 main categories (Fig. 1). Of these, 19 were related to traditional concepts of C-HP identification studies (Supplementary Table 1), 14 dealt with candidate diseases that could disrupt thermosensation or cause thermoregulation disorders, and 99 focused on candidate genes that could act as potential markers for C-HP identification (Supplementary Table 2).
- 2. Clinical studies implementing traditional medicine concepts of C-HPs
- A marked difference was observed between the C-HPs of patients with rheumatoid arthritis (RA) in multiple aspects such as immune function, C-reactive protein (CRP), rheumatoid factor, dehydroepiandrosterone sulfate levels, hypothalamic pituitary adrenal axis functionality, and muscle catabolism [14–16]. Furthermore, the disease activity score of 28 joints, erythrocyte sedimentation rate, white blood cell count, platelet count, albumin level, and globulin level differed significantly between the 2 groups [15,16]. Specifically, the heat pattern of patients with RA showed elevated inflammatory markers and was mainly influenced by interleukin-33 [17]. Furthermore, these patients showed significant upregulation of apoptosis-related genes and exhibited an accelerated rate of protein and collagen breakdown [18].
- Notably, neuroendocrine-immune network analysis indicated that toll-like receptor signaling was predominantly implicated in cold patterns of patients with RA [19,20]. In contrast, the heat pattern in patients with RA was associated with an array of pathways, including calcium signaling, cell adhesion, peroxisome proliferator-activated receptor signaling, and T cell proliferation [21–24].
- In patients with non-small cell lung cancer exhibiting a cold pattern, the prevalence of epidermal growth factor receptor (EGFR) gene mutations were significantly higher than that in patients with a non-cold pattern (p = 0.003) [7]. In patients with a non-cold pattern, a markedly elevated proportion of effector memory CD8 T cells (p = 0.015), and a higher proportion of terminal effector CD8 T cells (p = 0.005) were observed [25]. One study reported that in cancer survivors with cancer-related fatigue, moxibustion treatment was notably beneficial for patients with a cold pattern than in those with a heat pattern [26].
- According to a recent study, individuals in the non-cold pattern group tend to exhibit improved quality of life (QoL), body impedance analysis, and anthropometric measures [27]. Cold-heat scores have been determined to correlate with metabolic parameters such as body weight, body mass index, and body surface area, but these associations were relatively low (0.15–0.24) [28]. Lipid components, except for high-density lipoprotein, have been reported to be elevated in the heat pattern group compared with those in the cold pattern group [29]. Moreover, a strong relationship was observed between the heat pattern and metabolic syndrome (OR = 1.653) [29].
- One study reported a higher prevalence of the cold pattern (n = 35) than heat pattern (N = 5) among patients with asthma. Moreover, immunoglobulin E levels were over 4 times higher in patients classified under the cold pattern than in those classified under the heat pattern [30].
- The impact of C-HP on QoL, including physical, mental, and functional aspects is substantial. In a study involving both survey data and medical histories, individuals with a cold pattern showed lower QoL and metabolic function, and a more prevalent disease history than those with a heat pattern (p < 0.05) [31]. Sleep quality was reported to be notably poorer in the cold pattern group (p < 0.001), as evidenced by shorter sleep duration and lower sleep quality [32].
- 3. Application of the C-HP concept to thermoregulation-related disorders
- Thyroid dysfunction, a wide-spectrum endocrine disorder including both hypothyroidism and hyperthyroidism, presents as a unique set of challenges to the temperature-regulating capacity of the body. In individuals with hypothyroidism, a decrease in metabolic rate often results in reduced heat generation. This reduction compromises the innate thermoregulatory activities of the body, causing symptoms such as aversion to cold temperature. This indicates a problem with thermoregulation, which conflicts with the existing adaptive systems designed to generate heat. Conversely, hyperthyroidism accelerates metabolic processes which lead to excessive heat production. This results in symptoms such as heat intolerance and an excessive sweating, as the thermogenic activity of the body is increased, generating heat even when not required. Regardless of reduced heat production in hypothyroidism or excessive production of heat in hyperthyroidism, thyroid dysfunction disrupts the maintenance of heat homeostasis [33,34].
- Cold-induced sweating syndrome (CISS) is a rare genetic disorder characterized by excessive sweating after exposure to cold temperatures or during consumption of meals. It is caused by mutations in the cytokine receptor-like factor-1 (CRLF1) gene. Patients with CISS show high cold sensitivity, which is often described as feeling chilly. This sensation primarily originates from sweating, a critical thermoregulatory response that ensures that the body maintains an appropriate temperature. However, in CISS, this natural response is triggered by cold stimuli instead of heat, which results in an excessive sweating response which is inconsistent with normal thermoregulatory function [35–40].
- Sickle cell disease (SCD) is an inherited red blood cell disorder characterized by abnormally shaped red blood cells. This is caused by hemoglobin S which polymerizes under low-oxygen conditions, and leads to the deformation of red blood cells into a sickle or crescent shape. These sickle cells have reduced flexibility leading to the occlusion of small blood vessels and impaired oxygen delivery to tissues. Notably, cold sensitivity increases in individuals with this disease. These findings suggest that patients with SCD are hypersensitive to cold stimuli [41].
- Patients with Raynaud’s syndrome exhibit a critical disruption in thermoregulation, whereby there is significantly reduced capillary blood flow in both warm and cold environments compared with normal individuals. This impaired capillary flow, which is critical for thermoregulation, is further reduced during sympathetic stimulation, a key component of the temperature control mechanism in the body. Notably, treatment with reserpine (a drug used for the treatment of high blood pressure) improves this compromised capillary flow, underscoring the substantial impact of the disease on the temperature-regulating ability of the body [42,43].
- Cold urticaria is a common skin condition triggered by cold weather or a body temperature that is primarily caused by an abnormal immune response, and leads to inflammation when the skin is exposed to the cold. The immune system releases substances that cause symptoms such as hives, swelling, or even severe allergic reactions. Importantly, cold urticaria disrupts normal thermoregulation, leading to these symptoms. These symptoms often disappear within an hour of warming the skin. Currently, treatment involves avoiding the cold, taking antihistamines, and sometimes taking a drug called omalizumab [44,45].
- Familial cold autoinflammatory syndrome (FCAS) is an autosomal dominant disorder reported primarily in North American and European populations. It is characterized by a substantial impact on thermoregulation due to mutations particularly in the nucleotide-binding domain, leucine-rich-containing family, pyrin domain-containing-3 gene (NALP3). Unlike typical bodily responses to cold, individuals with FCAS experience rashes, low-grade fever, and joint pain within 1–2 hours of cold exposure, underlining the dysregulation of temperature-sensitive inflammatory pathways. This syndrome not only manifests with symptoms of the skin and musculoskeletal system, but it also carries the risk of rare, but serious, outcomes such as renal disease from AA amyloidosis, indicating that disruptions in thermal homeostasis can have far-reaching clinical consequences [46].
- 4. Key genes related to thermoregulation in the concept of C-HPs
- In mammals, including humans, brown adipose tissue (BAT) plays a key role in thermoregulation. Unlike white adipose tissue which stores energy, BAT specializes in using energy for heat production, a process known as thermogenesis. This capacity is largely attributed to the presence of the uncoupling protein 1 (UCP1) gene in BAT mitochondria. during adenosine triphosphate synthesis, UCP1 facilitates oxidative phosphorylation leading to heat generation rather than adenosine triphosphate production. Upon exposure to cold conditions, activation of the sympathetic nervous system leads to the release of norepinephrine, which binds to beta-adrenergic receptors on BAT cells. These events trigger intracellular signaling cascades, resulting in UCP1 activation and heat production (Supplementary Table 2).
- BAT plays an important role in metabolic regulation beyond heat production. Increasing evidence suggests that activity in BAT influences glucose homeostasis and lipid metabolism, potentially offering therapeutic avenues for obesity, diabetes, and related metabolic disorders [47–49]. Moreover, recent advances in imaging techniques have demonstrated the presence of functional (metabolically active) BAT in adult humans, where it was previously thought to be inactive or absent, highlighting the role of BAT in human thermoregulation and metabolism and its potential as a target for therapeutic intervention [50]. Although UCP1 is a key gene in BAT activation, other genes (UCP3 [51–53], PGC-1α [52,54–59], PRDM16 [50,60–62], SCD1 [63], CTR5 [64], KLF9 [54], AIFM2 [65], FAM195A [66], ADH5 [67], TG2 [68], PEX13 [58], SOX4 [62], and ORMDL3 [69]) also contribute to UCP1 expression and BAT activation.
- Transient receptor potential (TRP) channels are a diverse family of ion channels that respond to various stimuli including temperature changes. Some members of the TRP family known as “thermo-TRPs” are sensitive to temperature changes and serve as the primary thermosensors of the body. Among the TRP family, transient receptor potential cation channel subfamily M (TRPM) member 8 is known as the cold and menthol receptor, which is activated by temperatures 8–28 °C and is mainly found in the sensory neurons. TRPM8 activation can induce a cold sensation and cold-induced analgesia. Transient receptor potential cation channel subfamily A member 1 (TRPA1), known as the wasabi receptor, is activated by temperatures < 17 °C, and various natural compounds such as those found in wasabi, garlic, and onions, and it is mainly involved in nociception and inflammatory pathways (Supplementary Table 2). Transient receptor potential cation channel subfamily V (TRPV) Member 1 is a capsaicin receptor that is sensitive to temperatures > 43 °C, capsaicin (the spicy compound in hot chili peppers), and acidic conditions; its activation results in a sensation of burning pain. TRPV1 is critical to heat and pain sensation as well as body temperature regulation [70–78]. TRPV2 is activated by temperatures > 52 °C and is involved in high-threshold heat nociception [73,75,76]. TRPV3 is activated between 24–39 °C, is expressed in keratinocytes, and plays a role in maintaining skin homeostasis and hair morphogenesis [73,75,76]. TRPV4 is activated between 25–34 °C, is found in multiple tissues, and is involved in various physiological processes [73,75,76]. TRPM2, TRPM3, and ANO1 have also been found to function as thermosensors [76]. TRP channels also play important roles in inflammation. Notably, TRPV1, TRPA1, and TRPM8 channels are important mediators of inflammatory responses [78–80].
- Heat shock proteins are a family of proteins produced by all cells in response to stressful conditions such as elevated temperatures. They function as molecular chaperones, assist in the proper folding and stabilization of other proteins, prevent protein aggregation, and play crucial roles in protein homeostasis. In particular, heat shock protein 70 (HSP70) which has a mass of 70-kDa, are produced by cells in response to stressful conditions, including elevated temperatures. HSP70 has also been associated with thermoregulatory processes. When the body temperature increases, such as during fever, exercise, or exposure to a hot environment, HSP70 expression increases considerably. HSP70 helps protect and repair heat-damaged proteins, thereby promoting cellular survival under high-temperature conditions (Supplementary Table 2).
- Cold-inducible ribonucleic acid (RNA)-binding protein (CIRBP), originally discovered in vitro, was reported to be upregulated when cells were exposed to low temperatures. This protein was thus named for its ability to respond to cold stress [81]. The main function of CIRBP is to bind to RNA and guide its processing, thereby influencing the translation of certain genes in response to cold stress. CIRBP plays a crucial role in helping cells survive under cold conditions by ensuring the stability of specific messenger ribonucleic acid and facilitating its translation, subsequently leading to increased synthesis of proteins required for protecting cells against cold stress [82–84]. Specifically, exposure to cold stress triggers upregulation of specificity protein 1, and the subsequent increase in expression of CIRBP. This in turn leads to the production of extracellular CIRBP, which triggers damage-associated molecular pattern-mediated inflammation [84].
- In addition to the abovementioned genes, the expression of several other genes is altered upon exposure to thermal stress. A murine in vivo study showed that cold exposure led to an increase in the messenger ribonucleic acid expression levels of cytochrome P450, family 1, subfamily A, polypeptide 1 (CYP1A1) [85]. Additionally, studies conducted both in vitro and in vivo have reported elevated RNA binding motif 3 (RBM3) expression upon cold exposure [73,86,87]. Other genes (COMT, FAAH [73,86,87] and OPRD1 [74]) have also been shown to respond to thermal stress, thereby indicating their potential as candidate genes for further exploration in the context of thermal regulation.
- 5. GO and gene-set enrichment analysis
- Candidate genes were identified and screened in this review and their details are provided in Supplementary Table 2. To identify the underlying biological processes and functions associated with these genes, GO and gene-set enrichment analysis (GSEA) was conducted on 30 candidate genes using the Kyoto encyclopedia of genes and genomes database (Fig. 2 and Fig. 3). Categorization of the screened genes according to the number of publications revealed a distinct focus of studies on UCP1 and TRP genes (Fig. 2A). Following categorization of the results, as depicted in Fig. 2B, the most highly correlated processes involving thermoregulation-related genes were ranked as follows: (1) localization, (2) responses to stimuli; and (3) homeostatic processes. This ranking implies that the differences in responding to external stresses for maintaining homeostasis may be attributed to the categorization feature. Collectively, these thermoregulatory functions may have originated from variations in homeostatic processes. GSEA revealed a strong association between the regulation of TRP channels and inflammatory mediators based on the candidate genes of C-HP (p < 0.001, Fig. 2C).
Results
2.1. Rheumatoid arthritis
2.2. Cancer
2.3. Metabolic syndrome
2.4. Asthma
2.5. Quality of life
3.1. Thyroid dysfunction
3.2. Cold-induced sweating syndrome
3.3. Sickle cell disease
3.4. Raynaud’s syndrome
3.5. Cold urticaria
3.6. Familial cold autoinflammatory syndrome
4.1. Uncoupling protein 1
4.2. Transient receptor potential channels
4.3. Heat shock protein
4.4. Cold-inducible ribonucleic acid-binding protein
4.5. Other genes
- In this review, we aimed to synthesize traditional medicine diagnostic methods with modern analytical approaches in the context of C-HPs. Through an extensive examination of various studies, clinical and molecular characteristics of C-HPs in TEAM were extracted. A comprehensive investigation of conditions and diseases influenced by thermoregulation revealed potential factors that could be used to distinguish C-HPs. This review provides insights into the molecular mechanisms and genetic factors influencing C-HPs to emphasize the potential for integration into personalized custom care medicine.
- Clinical studies on RA, cancer, metabolic syndrome, asthma, and QoL in relation to C-HPs were analyzed. In RA, differences in clinical [14–16] and inflammatory markers like CRP and interleukin-33 [17] between C-HPs were observed, suggesting a potential for personalized treatment that targets specific inflammatory signaling pathways, such as toll-like receptor signaling in cold patterns [19,20], and calcium and peroxisome proliferator-activated receptor signaling in heat patterns [21–24]. In cancer, epidermal growth factor receptor mutations were more prevalent in patients with cold patterns [7], and the immune response in these patients differed significantly from those with non-cold patterns. This underlines the importance of C-HPs in cancer treatment, especially with the emergence of promising treatments such as immune checkpoint inhibitors, of which the efficacy may be further improved through a synergistic combination of traditional medicine concepts and modern medicine. A previous study showed no significant difference in immune checkpoint inhibitor responsiveness between cold and non-cold patterns [25]; however, a significant difference was observed in the proportion of effector memory CD8 T cells and terminal effector CD8 T cells, suggesting a distinct immune response between the 2 groups. Recent studies have also shown that hot or cold characterization of tumors is important for clinical therapeutic outcomes [88–90]. These conditions are closely associated with various factors such as immune properties, tumor microenvironment, and cell signaling pathways. Furthermore, remarkable variance in body mass index, body surface area, and other metabolic parameters in metabolic syndrome has been observed between C-HPs, signifying the necessity for pattern-specific treatment protocols [28]. Notably, lipid components which play roles in inflammatory processes, are elevated in the heat-pattern group, further highlighting the relationship between metabolic dysregulation and inflammation [29].
- The review also included disorders related to thermoregulation, such as thyroid dysfunction, CISS, SCD, Raynaud’s syndrome, cold urticaria, and FCAS. Thyroid dysfunction, particularly hypothyroidism and hyperthyroidism, showed similarities with C-HPs symptoms and classifications. Decreased fever, associated with hyperthyroidism, corresponds to a cold pattern, whereas increased temperature, commonly observed in hyperthyroidism, corresponds to a hot pattern [33,34]. For example, in thyroid dysfunction, hyperthyroidism often leads to conditions such as Graves’ disease, which is known to induce elevated levels of thyroid hormone secretion, resulting in increased body temperature and inflammatory responses [91]. Hashimoto’s thyroiditis, also known as chronic lymphocytic or autoimmune thyroiditis, is another notable example; it is the most prevalent form of inflammatory thyroid disease and typically, the root cause of hypothyroidism [92]. While Graves’ disease is associated with overproduction of thyroid hormones which increase body temperature and inflammation, and Hashimoto’s thyroiditis leads to a deficiency in thyroid hormones often manifesting in lower body temperatures. Similarly, the abnormal immune responses observed in cold urticaria [44,45], and the vascular impairments observed in Raynaud’s syndrome [42 43] both involve inflammatory mechanisms that compromise normal thermoregulatory function. Collectively, these findings highlight the homeostasis of immune functions as a link between temperature-related disorders and broader clinical symptoms.
- Following this analysis, genes involved in thermoregula-tion were selected to obtain a comprehensive understanding of C-HPs. The results highlight the molecular biomarkers for C-HP identification. UCP1, which is essential for the thermogenic activity of BAT, has emerged as a promising biomarker because of its dual function in thermoregulation and metabolic regulation. Recent research has indicated that adipose tissue is an important mediator of chronic low-grade inflammation, contributing to metabolic diseases, and complications in obesity through the secretion of inflammatory adipokines and cytokines [93]. Importantly, BAT has been linked to anti-inflammatory activity, suggesting that UCP1 is involved in mediating inflammation [94]. The metabolic role of UCP1 provides a strong basis for its inclusion in C-HP identification. The TRP channel family, along with its thermally sensitive members, particularly TRPM8 and TRPV1, expands the range of molecular markers for exploring C-HPs. These channels may also offer an exceptional framework for correlating sensory thermal experiences. These channels modulate immune responses, implicating them in both thermoregulatory and inflammatory processes. HSP70 [83,86,95–97], which provides protection under heat stress, and CIRBP [81] which mediates RNA processing during cold stress, also highlight cellular adaptations, and both have been shown to exert anti-inflammatory effects [84]. Furthermore, the results of this review suggest that other candidate genes (COMT, FAAH, and OPRD1) may respond to thermal stress. These thermoregulation-related genes are closely associated with immune functions implicated in C-HPs.
- GO categorization performed for this review highlighted the importance of cellular localization, emphasizing its role within the complex matrix of cellular processes, where the importance of “response to stimulus” mechanisms facilitate C-HP differentiation in TEAM. The variability in individual responses to external stimuli has long been recognized as a means for identifying C-HPs. These findings confirm the traditional medicine perspectives and implicate candidate genes as potential mediators of diverse physiological responses. Moreover, homeostatic processes are consistent with the basic principles of TEAM, which emphasize internal physiological balance.
- Furthermore, GSEA revealed a robust interaction between temperature sensitivity and inflammatory pathways. This finding could have important implications for understanding thermoregulatory mechanisms and their effects on the immune system whereby TRP channels may modulate inflammatory mediators in response to temperature changes. This interrelationship suggests that thermoregulation and inflammation do not exist separately but may be 2 interconnected processes that influence each other. Furthermore, a recent 2,000 sample cohort study supported the link between genetic variations related to cold sensitivity and inflammatory pathways, notably through CIRBP expression [84]. This finding is consistent with GSEA performed for this review, which revealed a significant association between the regulation of TRP channels and inflammatory mediators for the candidate genes C-HP inflammatory pathways (p < 0.001).
- Despite the promising insights provided, this study had several limitations that must be acknowledged. Firstly, although this review included a comprehensive range of C-HP studies, the inherent heterogeneity of these studies could introduce a potential bias. Additionally, our reliance on previously published data limited our capacity to control for variables that may not have been considered in the original studies. Secondly, the candidate diseases and genes that were presented for C-HP identification, although pivotal, represent only a fraction of the possible molecular players involved in thermoregulation and inflammation. Additional genes and pathways that may play substantial roles in C-HP expression remain unidentified. Our study also primarily focused on genetic and molecular markers which although important, are only part of the broader biological and environmental landscape influencing C-HP differentiation. Factors such as individual lifestyle, diet, and external environmental influences, which may have a noteworthy impact on C-HP have not been extensively explored.
Discussion
- In conclusion, this study revealed an important association between the concept of C-HPs in TEAM and inflammation-related pathways across clinical and preclinical studies based on thermosensation and thermoregulation. We anticipate that this review will drive further research on the traditional medicine concept of C-HPs from an immunological perspective and contribute to expanding the framework for implementing personalized medicine.
Conclusion
Supplementary Material
-
Author Contributions
Conceptualization: SL. Methodology: SL. Data analysis: YK and JL. Writing original draft: YK. Writing - review and editing: JYL and SL.
-
Conflicts of Interest
JL and SL are a representative of BinaryTunerS Inc. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
-
Funding
This work was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, funded by the Ministry of Health and Welfare, Republic of Korea (grant no.: HF23C0040).
Article information
Data Availability


- [1] Liu J, Feng W, Peng C. A song of ice and fire: cold and hot properties of traditional Chinese medicines. Front Pharmacol 2020;11:598744. ArticlePubMedPMC
- [2] Ji GY. Clinical practice guideline of Korean medicine: the pattern identification of the eight principles. Gyeongsan (Korea), National Institute Korean Medicine Development;, 2023, [in Korean].
- [3] World Health Organization Regional Office for the Western P. WHO international standard terminologies on traditional medicine in the western pacific region. Manila (Philiphine), WHO Regional office For the Western Pacific, 2007.
- [4] Park YJ, Nam JH, Yim MH, Kim H, Kim JY. A study on the diagnostic elements of cold-heat pattern identification by Korean medicine doctors: association with objective and subjective body temperature. Evid Based Complement Alternat Med 2017;2017:7593056. ArticlePubMedPMCPDF
- [5] Lee BJ, Lee JC, Nam J, Kim JY. prediction of cold and heat patterns using anthropometric measures based on maChine learning. Chin J Integr Med 2018;24(1):16−23.ArticlePubMedPDF
- [6] Seca S, Franconi G. Understanding Chinese medicine patterns of rheumatoid arthritis and related biomarkers. Medicines (Basel) 2018;5(1):17. ArticlePubMedPMC
- [7] Zhu YJ, Zhang HB, Liu LR, Liu YH, Zhang FL, Bai JP, et al. Yin-cold or yang-heat syndrome type of traditional Chinese medicine was associated with the epidermal growth factor receptor gene status in non-small cell lung cancer patients: confirmation of a TCM concept. Evid Based Complement Alternat Med 2017;2017:7063859. ArticlePubMedPMCPDF
- [8] Lee S. Systems biology - a pivotal research methodology for understanding the mechanisms of traditional medicine. J Pharmacopunct 2015;18(3):11−8.ArticlePubMedPMC
- [9] Chen G, Xue WD, Zhu J. Full genetic analysis for genome-wide association study of fangji: a powerful approach for effectively dissecting the molecular architecture of personalized traditional Chinese medicine. Acta Pharmacol Sin 2018;39(6):906−11.ArticlePubMedPMCPDF
- [10] Hur Y-M, Yu H, Jin H-J, Lee S. Heritability of cold and heat patterns: a twin study. Twin Res Hum Genet 2018;21(3):227−32.ArticlePubMed
- [11] Binns D, Dimmer E, Huntley R, Barrell D, O’Donovan C, Apweiler R. Quickgo: a web-based tool for gene ontology searChing. Bioinformatics 2009;25(22):3045−6.ArticlePubMedPMCPDF
- [12] Kanehisa M, Furumichi M, Sato Y, Ishiguro-Watanabe M, Tanabe M. KEGG: integrating viruses and cellular organisms. Nucleic Acids Res 2020;49(D1):D545−51.ArticlePubMedPMCPDF
- [13] Fang Z, Liu X, Peltz G. Gseapy: a comprehensive package for performing gene set enrichment analysis in python. Bioinformatics 2022;39(1):btac757.. ArticlePubMedPMCPDF
- [14] van Wietmarschen HA, Dai W, Van Der Kooij AJ, Reijmers TH, Schroën Y, Wang M, et al. Characterization of rheumatoid arthritis subtypes using symptom profiles, clinical chemistry and metabolomics measurements. PLoS One 2012;7(9):E44331. ArticlePubMedPMC
- [15] Wang ZZ, Fang YF, Wang Y, Mu FX, Chen J, Zou QH, et al. Logistic regression analysis of damp-heat and cold-damp impeding syndrome of rheumatoid arthritis: a perspective in Chinese medicine. Chin J Integr Med 2012;18(8):575−81.ArticlePubMedPDF
- [16] Wang W, Guan J, Li Z, Wang X. Rheumatoid arthritis characteristics and classification of heat and cold patterns-an observational study. Heliyon 2023;9(2):E13439. ArticlePubMedPMC
- [17] Wang Y, Chen Z, Huang Y, Yafei L, Tu S. Prognostic significance of serum interleukins and soluble st2 in traditional Chinese medicine (TCM) syndrome-differentiated rheumatoid arthritis. Med Sci Monit 2018;24:3472−8.ArticlePubMedPMC
- [18] Van Wietmarschen H, Yuan K, Lu C, Gao P, Wang J, Xiao C, et al. Systems biology guided by Chinese medicine reveals new markers for sub-typing rheumatoid arthritis patients. J Clin Rheumatol 2009;15(7):330−7.ArticlePubMed
- [19] Cheng L, Yuanyan L, Cheng X, Miao J, Qinglin Z, Aiping L. Biological basis of cold and heat pattern of rheumatoid arthritis in traditional Chinese medicine. World Sci Tech 2010;12(5):814−7.Article
- [20] Wang M, Chen G, Lu C, Xiao C, Li L, Niu X, et al. Rheumatoid arthritis with deficiency pattern in traditional Chinese medicine shows correlation with cold and hot patterns in gene expression profiles. Evid Based Complement Alternat Med 2013;2013:248650. ArticlePubMedPMCPDF
- [21] Jiang M, Xiao C, Chen G, Lu C, Zha Q, Yan X, et al. Correlation between cold and hot pattern in traditional Chinese medicine and gene expression profiles in rheumatoid arthritis. Front Med 2011;5(2):219−28.ArticlePubMedPDF
- [22] Chen G, Lu C, Zha Q, Xiao C, Xu S, Ju D, et al. A network-based analysis of traditional Chinese medicine cold and hot patterns in rheumatoid arthritis. Complement Ther Med 2012;20(1–2):23−30.ArticlePubMed
- [23] Lu C, Niu X, Xiao C, Chen G, Zha Q, Guo H, et al. Network-based gene expression biomarkers for cold and heat patterns of rheumatoid arthritis in traditional Chinese medicine. Evid Based Complement Alternat Med 2012;2012:203043. ArticlePubMedPMCPDF
- [24] Lu C, Xiao C, Chen G, Jiang M, Zha Q, Yan X, et al. Cold and heat pattern of rheumatoid arthritis in traditional Chinese medicine: distinct molecular signatures indentified by microarray expression profiles in CD4-positive t cell. Rheumatol Int 2012;32(1):61−8.ArticlePubMedPMC
- [25] Choi Y, Kwon O, Choi CM, Jeong MK. A pilot study of whether the cold-heat syndrome type is associated with treatment response and immune status in patients with non-small cell lung cancer. Evid Based Complement Alternat Med 2021;2021:9920469. ArticlePubMedPMCPDF
- [26] Han K, Kim M, Kim EJ, Park YC, Kwon O, Kim AR, et al. Moxibustion for treating cancer-related fatigue: a multicenter, assessor-blinded, randomized controlled clinical trial. Cancer Med 2021;10(14):4721−33.ArticlePubMedPMCPDF
- [27] Lee E, Kim S, Lee S, Cha S, Lee Y, Mun S. An analysis of the relationship between the cold pattern and anthropometry, bio impedance analysis (bia) and quality of life in Jeju haenyeo. J Soc Prevent Korean Med 2016;20(3):67−74. [in Korean] https://koreascience.kr/article/JAKO201610236161750.page.
- [28] Mun S, Park K, Lee S. Association of cold-heat pattern and anthropometry/body composition in individuals between 50–80 years of age. J Physiol Pathol Korean Med 2020;34(4):209−14. [in Korean].Article
- [29] Park K-H, Kim S-H, Lee S, Bae KH. Analysis of the difference in the prevalence of metabolic syndrome according to sasang constitution and cold and heat pattern identification. J Intern Korean Med 2022;43(6):1063−74. [in Korean].ArticlePDF
- [30] Bhang Y-H, Kim J-H, Do H-Y, Kim M-A, Kim K-I, Lee B-J, et al. Deficiency-excess and cold-heat pattern identification and analysis of the characteristics of asthma patients. J Intern Korean Med 2017;38(6):955−70. [in Korean].ArticlePDF
- [31] Joo J-C, Lee S, Park SJ. Comparison of health status and mibyeong characteristics between cold syndrome and heat syndrome by cold heat syndrome differentiation score. J Korean Med 2018;39(1):13−21. [in Korean].Article
- [32] Seo B-N, Jeong K, Baek Y, Lee S. Study on the relationship between cold type and sleep quality in Koreans. J Physiol Pathol Korean Me 2021;35(1):42−6. [in Korean].Article
- [33] Gordon CJ, Becker P, Padnos B. Comparison of heat and cold stress to assess thermoregulatory dysfunction in hypothyroid rats. Am J Physiol Regul Integr Comp Physiol 2000;279(6):R2066−71.ArticlePubMed
- [34] Hwang MS, Hwang JH, Kang SY, Kang AN, Roh HS, Park YK. Effects study of aconiti lateralis radix preparata extract on the regulation of heat and cold in ptu-induced hypothyroidism rats. Korean J Herbology 2016;31(6):63−71. [in Korean].Article
- [35] Knappskog PM, Majewski J, Livneh A, Nilsen PT, Bringsli JS, Ott J, et al. Cold-induced sweating syndrome is caused by mutations in the crlf1 gene. Am J Hum Genet 2003;72(2):375−83.ArticlePubMedPMC
- [36] Crisponi L, Crisponi G, Meloni A, Toliat MR, Nurnberg G, Usala G, et al. Crisponi syndrome is caused by mutations in the CRLF1 gene and is allelic to cold-induced sweating syndrome Type 1. Am J Hum Genet 2007;80(5):971−81.ArticlePubMedPMC
- [37] Piras R, Chiappe F, Torraca IL, Buers I, Usala G, Angius A, et al. Expanding the mutational spectrum of CRLF1 in crisponi/CISS1 syndrome. Hum Mutat 2014;35(4):424−33.ArticlePubMed
- [38] Angius A, Uva P, Buers I, Oppo M, Puddu A, Onano S, et al. Bi-allelic mutations in KLHL7 cause a crisponi/CISS1-like phenotype associated with early-onset retinitis pigmentosa. Am J Hum Genet 2016;99(1):236−45.ArticlePubMedPMC
- [39] Agresta A, Fasciani R, Padua L, Petroni S, La Torraca I, Dickmann A, et al. Corneal alterations in crisponi/ciss1 syndrome: a slit-lamp biomicroscopy and in vivo confocal microscopy corneal report. Ophthalmic Genet 2017;38(1):83−7.ArticlePubMed
- [40] Schöning L, Loges NT, Nitschke Y, Höben IM, Röpke A, Crisponi L, et al. Generation of induced pluripotent stem cell lines from a crisponi/cold induced sweating syndrome type 1 individual. Stem Cell Res 2020;46:101820.
- [41] Brandow AM, Stucky CL, Hillery CA, Hoffmann RG, Panepinto JA. Patients with sickle cell disease have increased sensitivity to cold and heat. Am J Hematol 2013;88(1):37−43.ArticlePubMedPMC
- [42] Klein-Weigel P, Sander O, Reinhold S, Nielitz J, Steindl J, Richter J. Raynaud’s phenomenon: a vascular acrosyndrome that requires long-term care. Dtsch Arztebl Int 2021;118(Forthcoming):273−80.ArticlePubMedPMC
- [43] Heidrich Helmis, Fahrig Hövelmann, Vasa MJ. Clinical characteristics of primary, secondary and suspected secondary raynaud’s syndrome and diagnostic transition in the long-term follow-up. a retrospective study in 900 patients. Vasa Eur J Vasc Med 2008;37(Suppl 73):3−25.Article
- [44] Romanovsky AA. Skin temperature: its role in thermoregulation. Acta Physiol (Oxf) 2014;210(3):498−507.ArticlePubMedPMCPDF
- [45] Stocks JM, Taylor NA, Tipton MJ, Greenleaf JE. Human physiological responses to cold exposure. Aviat Space Environ Med 2004;75(5):444−57.PubMed
- [46] Hoffman HM, Wanderer AA, Broide DH. Familial cold autoinflammatory syndrome: phenotype and genotype of an autosomal dominant periodic fever. J Allergy Clin Immunol 2001;108(4):615−20.ArticlePubMedPMC
- [47] Zhao S, Mugabo Y, Ballentine G, Attane C, Iglesias J, Poursharifi P, et al. A/B-hydrolase domain 6 deletion induces adipose browning and prevents obesity and type 2 diabetes. Cell Rep 2016;14(12):2872−88.PubMed
- [48] Hepler C, Shao M, Xia JY, Ghaben AL, Pearson MJ, Vishvanath L, et al. Directing visceral white adipocyte precursors to a thermogenic adipocyte fate improves insulin sensitivity in obese mice. Elife 2017;6:e27669.. ArticlePubMedPMCPDF
- [49] Xu L, Li D, Li H, Zhang O, Huang Y, Shao H, et al. Suppression of obesity by melatonin through increasing energy expenditure and accelerating lipolysis in mice fed a high-fat diet. Nutr Diabetes 2022;12(1):42. ArticlePubMedPMCPDF
- [50] Nagano G, Ohno H, Oki K, Kobuke K, Shiwa T, Yoneda M, et al. Activation of classical brown adipocytes in the adult human perirenal depot is highly correlated with PRDM16-EHMT1 complex expression. PLoS One 2015;10(3):E0122584. ArticlePubMedPMC
- [51] Katsumata M, Matsumoto M, Kawakami S, Kaji Y. Effect of heat exposure on uncoupling protein-3 mrna abundance in porcine skeletal muscle. J Anim Sci 2004;82(12):3493−9.ArticlePubMed
- [52] Mollica MP, Lionetti L, Crescenzo R, Tasso R, Barletta A, Liverini G, et al. Cold exposure differently influences mitochondrial energy efficiency in rat liver and skeletal muscle. FEBS Lett 2005;579(9):1978−82.ArticlePubMed
- [53] Ribeiro MO, Bianco SD, Kaneshige M, Schultz JJ, Cheng SY, Bianco AC, et al. Expression of uncoupling protein 1 in mouse brown adipose tissue is thyroid hormone receptor-beta isoform specific and required for adaptive thermogenesis. Endocrinology 2010;151(1):432−40.ArticlePubMedPMC
- [54] Fan H, Zhang Y, Zhang J, Yao Q, Song Y, Shen Q, et al. Cold-inducible Klf9 regulates thermogenesis of brown and beige fat. Diabetes 2020;69(12):2603−18.ArticlePubMedPDF
- [55] Lee CH, Choi YA, Heo SJ, Song P. The effect of hyperbaric therapy on brown adipose tissue in rats. Int J Environ respublic Health 2021;18(17):9165. ArticlePubMedPMC
- [56] Lemecha M, Morino K, Imamura T, Iwasaki H, Ohashi N, Ida S, et al. Mir-4943p regulates mitochondrial biogenesis and thermogenesis through PGC1-A signalling in beige adipocytes. Sci Rep 2018;8(1):15096. PubMedPMC
- [57] Li F, Wu R, Cui X, Zha L, Yu L, Shi H, et al. Histone deacetylase 1 (HDAC1) negatively regulates thermogenic program in brown adipocytes via coordinated regulation of histone H3 lysine 27 (H3K27) deacetylation and methylation. J Biol Chem 2016;291(9):4523−36.ArticlePubMedPMC
- [58] Park WY, Park J, Lee S, Song G, Nam IK, Ahn KS, et al. PEX13 is required for thermogenesis of white adipose tissue in cold-exposed mice. Biochim Biophys Acta Mol Cell Biol Lipids 2022;1867(1):159046. ArticlePubMed
- [59] Zha L, Li F, Wu R, Artinian L, Rehder V, Yu L, et al. The histone demethylase UTX promotes brown adipocyte thermogenic program via coordinated regulation of H3K27 demethylation and acetylation. J Biol Chem 2015;290(41):25151−63.ArticlePubMedPMC
- [60] Kim S, Park JW, Lee MG, Nam KH, Park JH, Oh H, et al. reversine promotes browning of white adipocytes by suppressing mir-133a. J Cell Physiol 2019;234(4):3800−13.ArticlePubMedPDF
- [61] Liu W, Bi P, Shan T, Yang X, Yin H, Wang YX, et al. Mir-133a regulates adipocyte browning in vivo. Plos Genet 2013;9(7):e1003626.. ArticlePubMedPMC
- [62] Shen H, He T, Wang S, Hou L, Wei Y, Liu Y, et al. SOX4 promotes beige adipocyte-mediated adaptive thermogenesis by facilitating PRDM16-Ppary complex. Theranostics 2022;12(18):7699−716.ArticlePubMedPMC
- [63] Forney LA, Stone KP, Wanders D, Ntambi JM, Gettys TW. The role of suppression of hepatic SCD1 expression in the metabolic effects of dietary methionine restriction. Appl Physiol Nutr Metab 2018;43(2):123−30.ArticlePubMedPMC
- [64] Rao C, Huang D, Mao X, Chen R, Huang D, Huang K. The novel adipokine CTRP5 is a negative regulator of white adipose tissue browning the novel adipokine CTRP5 is a negative regulator of white adipose tissue browning. Biochem Biophys Res Commun 2019;510(3):388−94.PubMed
- [65] Nguyen HP, Yi D, Lin F, Viscarra JA, Tabuchi C, Ngo K, et al. Aifm2, A NADH oxidase, supports robust glycolysis and is required for cold- and diet-induced thermogenesis. Mol Cell 2020;77(3):600−17e4.ArticlePubMedPMC
- [66] Cannavino J, Shao M, An YA, Bezprozvannaya S, Chen S, Kim J, et al. regulation of cold-induced thermogenesis by the RNA binding protein FAM195A. Proc Natl Acad Sci U S A 2021;118(23):e2104650118. ArticlePubMedPMC
- [67] Sebag SC, Zhang Z, Qian Q, Li M, Zhu Z, Harata M, et al. ADH5-mediated NO bioactivity maintains metabolic homeostasis in brown adipose tissue. Cell Rep 2021;37(7):110003. ArticlePubMedPMC
- [68] Lénárt K, Bankó C, Ujlaki G, Póliska S, Kis G, Csősz É, et al. Tissue transglutaminase knock-out preadipocytes and beige cells of epididymal fat origin possess decreased mitochondrial functions required for thermogenesis. Int J Mol Sci 2022;23(9):5175. ArticlePubMedPMC
- [69] Song Y, Zan W, Qin L, Han S, Ye L, Wang M, et al. Ablation of ORMDL3 impairs adipose tissue thermogenesis and insulin sensitivity by increasing ceramide generation. Mol Metab 2022;56:101423. ArticlePubMedPMC
- [70] Bockhart V, Constantin CE, Häussler A, Wijnvoord N, Kanngiesser M, Myrczek T, et al. Inhibitor kappab kinase beta deficiency in primary nociceptive neurons increases TRP channel sensitivity. J Neurosci 2009;29(41):12919−29.ArticlePubMedPMC
- [71] Cao Z, Balasubramanian A, Marrelli SP. Pharmacologically induced hypothermia via TRPV1 channel agonism provides neuroprotection following ischemic stroke when initiated 90 min after reperfusion. Am J Physiol Regul Integr Comp Physiol 2014;306(2):R149−56.ArticlePubMedPMC
- [72] Elitt CM, Mcilwrath SL, Lawson JJ, Malin SA, Molliver DC, Cornuet PK, et al. Artemin overexpression in skin enhances expression of TRPV1 and TRPA1 in cutaneous sensory neurons and leads to behavioral sensitivity to heat and cold. J Neurosci 2006;26(33):8578−87.ArticlePubMedPMC
- [73] Fujita T, Higashitsuji H, Higashitsuji H, Liu Y, Itoh K, Sakurai T, et al. TRPV4-dependent induction of a novel mammalian cold-inducible protein SRSF5 as well as CIRP and RBM3. Sci Rep 2017;7:2295. ArticlePubMedPMCPDF
- [74] Kim H, Mittal DP, Iadarola MJ, Dionne RA. Genetic predictors for acute experimental cold and heat pain sensitivity in humans. J Med Genet 2006;43(8):e40.. ArticlePubMedPMC
- [75] Nozadze I, Tsiklauri N, Gurtskaia G, Tsagareli MG. Role of thermo TRPA1 and TRPV1 channels in heat, cold, and mechanical nociception of rats. Behav Pharmacol 2016;27(1):29−36.ArticlePubMed
- [76] Tan CH, Mcnaughton PA. The TRPM2 ion channel is required for sensitivity to warmth. Nature 2016;536(7617):460−3.ArticlePubMedPMCPDF
- [77] Voets T, Droogmans G, Wissenbach U, Janssens A, Flockerzi V, Nilius B. The principle of temperature-dependent gating in cold- and heat-sensitive TRP channels. Nature 2004;430(7001):748−54.ArticlePubMedPDF
- [78] Simões RR, Coelho ID, Junqueira SC, Pigatto GR, Salvador MJ, Santos AR, et al. Oral treatment with essential oil of hyptis spicigera lam. (lamiaceae) reduces acute pain and inflammation in mice: potential interactions with transient receptor potential (TRP) ion channels. J Ethnopharmacol 2017;200:8−15.ArticlePubMed
- [79] Liu H, Liu Q, Hua L, Pan J. Inhibition of transient receptor potential melastatin 8 alleviates airway inflammation and remodeling in a murine model of asthma with cold air stimulus. Acta Biochim Biophys Sin (Shanghai) 2018;50(5):499−506.ArticlePubMedPDF
- [80] Yamaki S, Chau A, Gonzales L, Mckemy DD. Nociceptive afferent phenotyping reveals that transient receptor potential ankyrin 1 promotes cold pain through neurogenic inflammation upstream of the neurotrophic factor receptor gfrα3 and the menthol receptor transient receptor potential melastatin 8. Pain 2021;162(2):609−18.ArticlePubMedPMC
- [81] Leeuw De. F, Zhang T, Wauquier C, Huez G, Kruys V, Gueydan C. The cold-inducible rna-binding protein migrates from the nucleus to cytoplasmic stress granules by a methylation-dependent mechanism and acts as a translational repressor. Exp Cell Res 2007;313(20):4130−44.PubMed
- [82] Xia Z, Zheng X, Zheng H, Liu X, Yang Z, Wang X. Cold-inducible RNA-binding protein (CIRP) regulates target mrna stabilization in the mouse testis. FEBS Letters 2012;586(19):3299−308.ArticlePubMedPDF
- [83] Kaneko T, Kibayashi K. Mild hypothermia facilitates the expression of cold-inducible RNA-binding protein and heat shock protein 70.1 in mouse brain. Brain Res 2012;1466:128−36.ArticlePubMed
- [84] Kim SY, Ban H-J, Lee S, Jin HJ. Regulation of CIRP by genetic factors of SP1 related to cold sensitivity. Front Immunol 2022;13:994699. ArticlePubMedPMC
- [85] Perepechaeva ML, Sidorova YA, Grishanova AY. Effect of cold stress on expression of genes for the ahr-dependent pathway of CYP1 regulation in rat liver. Bull Exp Biol Med 2006;141(3):315−8.ArticlePubMedPDF
- [86] Sonna LA, Kuhlmeier MM, Khatri P, Chen D, Lilly CM. A microarray analysis of the effects of moderate hypothermia and rewarming on gene expression by human hepatocytes (Hepg2). Cell Stress Chaperones 2010;15(5):687−702.ArticlePubMedPMCPDF
- [87] Sonna LA, Kuhlmeier MM, Carter HC, Hasday JD, Lilly CM, Fairchild KD. Effect of moderate hypothermia on gene expression by THP-1 cells: a DNA microarray study. Physiol Genomics 2006;26(1):91−8.ArticlePubMed
- [88] Li JX, Huang JM, Jiang ZB, Li RZ, Sun A, Lai-Han Leung E, et al. Current clinical progress of PD-1/PD-L1 immunotherapy and potential combination treatment in non-small cell lung cancer. Integr Cancer Ther 2019;18:1534735419890020. ArticlePubMedPMCPDF
- [89] Yu YX, Wang S, Liu ZN, Zhang X, Hu ZX, Dong HJ, et al. Traditional Chinese medicine in the era of immune checkpoint inhibitor: theory, development, and future directions. Chin Med 2023;18(1):59. ArticlePubMedPMCPDF
- [90] Lu Y, Yuan X, Wang M, He Z, Li H, Wang J, et al. Gut microbiota influence immunotherapy responses: mechanisms and therapeutic strategies. J Hematol Oncol 2022;15(1):47. ArticlePubMedPMCPDF
- [91] Davies TF, andersen S, Latif R, Nagayama Y, Barbesino G, Brito M, et al. Graves’ disease. Nat Rev Dis Primers 2020;6(1):52. ArticlePubMedPDF
- [92] Resende De Paiva C, Grønhøj C, Feldt-Rasmussen U, Von Buchwald C. Association between hashimoto’s thyroiditis and thyroid cancer in 64,628 patients. Front Oncol 2017;7:53. PubMedPMC
- [93] Kawai T, Autieri MV, Scalia R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am J Physiol Cell Physiol 2021;320(3):C375−91.ArticlePubMedPMC
- [94] Omran F, Christian M. Inflammatory signaling and brown fat activity. Front Endocrinol (Lausanne) 2020;11:156. ArticlePubMedPMC
- [95] Nielsen MM, Overgaard J, Sørensen JG, Holmstrup M, Justesen J, Loeschcke V. Role of HSF activation for resistance to heat, cold and high-temperature knock-down. J Insect Physiol 2005;51(12):1320−9.ArticlePubMed
- [96] Ren J, Liu C, Zhao D, Fu J. The role of heat shock protein 70 in oxidant stress and inflammatory injury in quail spleen induced by cold stress. Environ Sci Pollut Res 2018;25(21):21011−23.ArticlePDF
- [97] Szpotowicz-Czech B, Wiecek M, Szymura J, Maciejczyk M, Szygula Z. Changes in chosen immune system indicators and the level of HSP-70 after single whole-body cryostimulation in healthy men. Cent Eur J Immunol 2018;43(2):186−93.ArticlePubMedPMC
References
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite