Articles
- Page Path
- HOME > Perspect Integr Med > Volume 2(3); 2023 > Article
-
Review Article
An Umbrella Review of Systematic Reviews for Chuna (or Tuina) Manual Therapy on Musculoskeletal Disorders -
Doori Kim1
 , Gil Geun Baek2, Byung-Cheul Shin3,*
, Gil Geun Baek2, Byung-Cheul Shin3,* -
Perspectives on Integrative Medicine 2023;2(3):142-154.
DOI: https://doi.org/10.56986/pim.2023.10.002
Published online: October 23, 2023
1Jaseng Spine and Joint Research Institute, Jaseng Medical Foundation, Seoul, Republic of Korea
2Jaseng Hospital of Korean Medicine, Seoul, Republic of Korea
3Department of Korean Rehabilitation Medicine, Pusan National University Korean Medicine Hospital, Yangsan, Republic of Korea
- *Corresponding author: Byung-Cheul Shin. Department of Korean Rehabilitation Medicine, Pusan National University Korean Medicine Hospital, 49 Busandaehak-ro, Mulgeum-eup, Yangsan, Gyeongsangnam-do 50612, Republic of Korea, Email: drshinbc@pusan.ac.kr
©2023 Jaseng Medical Foundation
This is an open access article under the CC BY-NC license (http://creativecommons.org/licenses/by-nc/4.0/).
- 1,089 Views
- 33 Download
- 1 Crossref
Abstract
-
Background
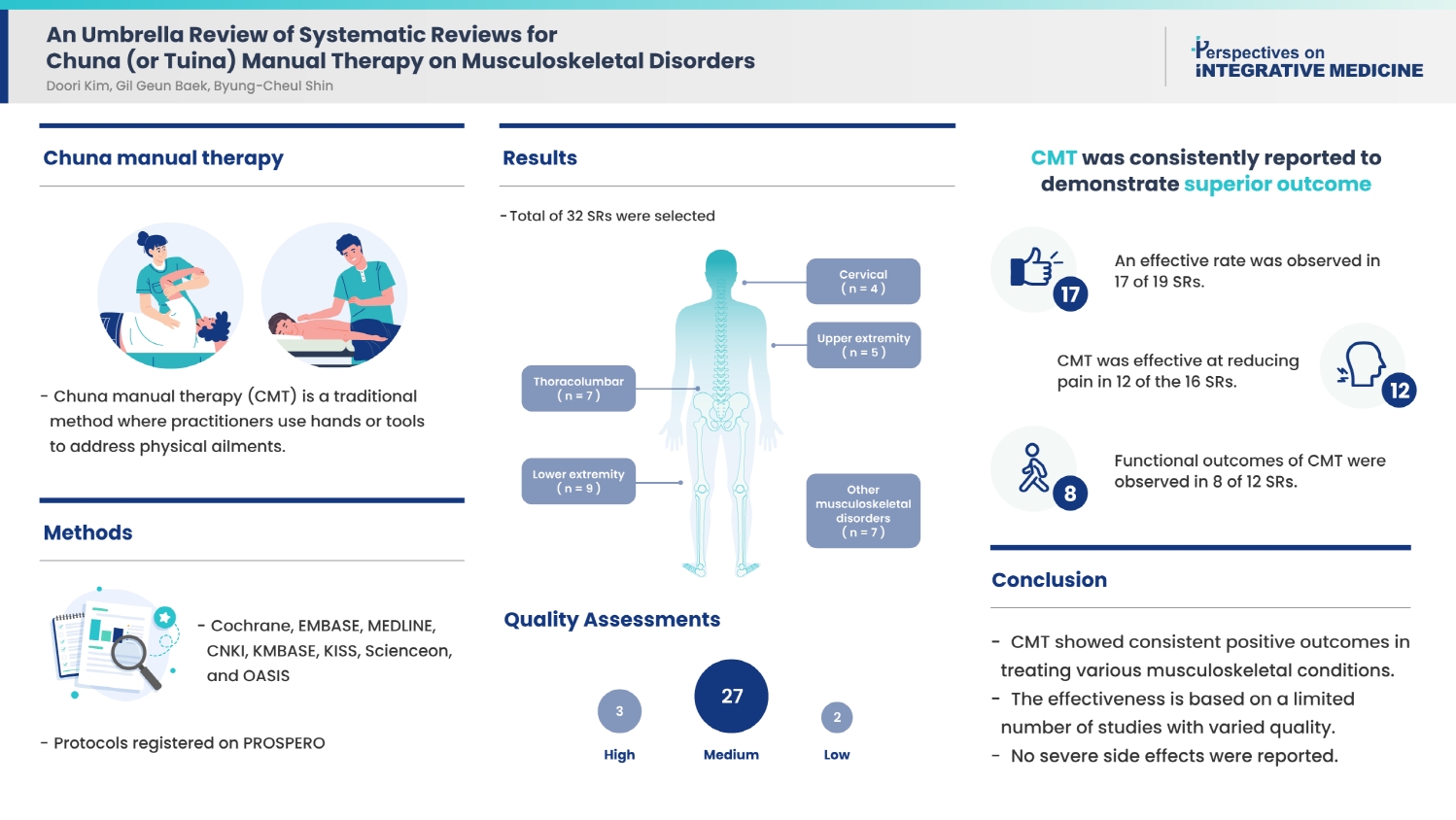
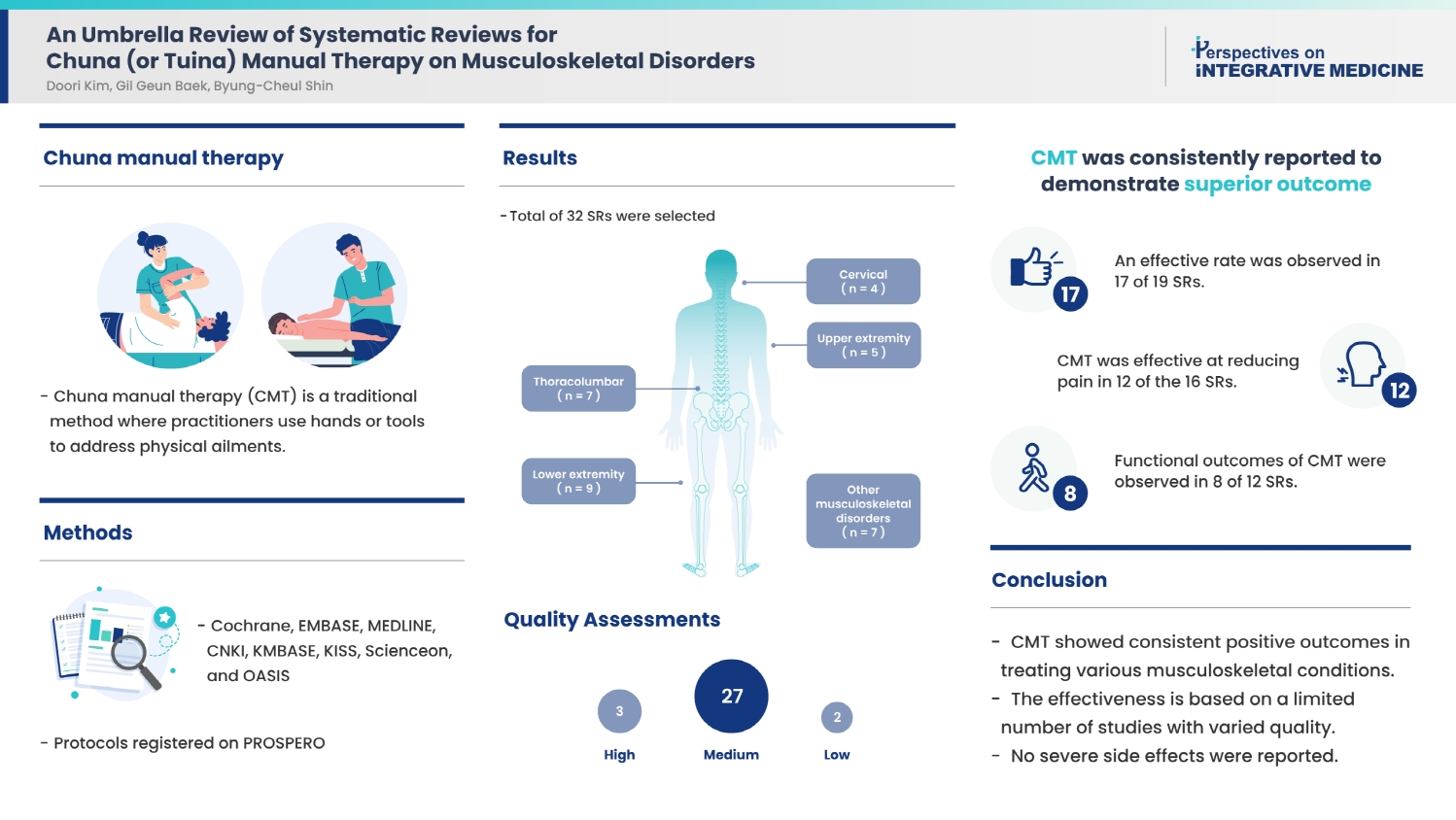
- To provide clinicians with reliable evidence an umbrella review of systematic reviews (SRs) on Chuna manual therapy (CMT) for musculoskeletal disorders was performed to synthesize important outcomes.
-
Methods
- There were eight databases (Cochrane, EMBASE, MEDLINE, CNKI, KMBASE, KISS, Scienceon, and OASIS) searched as well as the international database Prospective Register of Systematic Reviews in health and social care until August 2023. SRs of randomized controlled trials involving patients with musculoskeletal conditions, limited to interventions explicitly labeled as “Chuna” or “Tuina” in English, Chinese, or Korean language were retrieved. Two reviewers independently conducted selection and data extraction, and SR quality was assessed using A Measurement Tool to Assess Systematic Reviews tool (low, medium, or high quality).
-
Results
- This review included 32 SRs, categorized by cervical (n = 4), thoracolumbar (n = 7), upper extremity (n = 5), lower extremity (n = 9), and other musculoskeletal disorders (n = 7). Quality assessments determined that three SRs were of “high” quality, two were “low” quality, and the remaining SRs were of “medium” quality. CMT was consistently reported to demonstrate superior outcomes: an effective rate was observed in 17 of 19 SRs, CMT was effective at reducing pain in 12 of the 16 SRs, and functional outcomes of CMT were observed in 8 of 12 SRs. No serious adverse events were reported.
-
Conclusion
- CMT may be a safe and effective treatment for various musculoskeletal disorders based on the limited number of studies and the low quality of included SRs.
- Musculoskeletal disorders represent an important societal and economic concern due to their chronic nature, the extensive burdens they impose on individuals and society, and the severe physical pain and disability they cause [1–3]. Consequently, as the elderly population increases, and lifestyles changes in the population lead to physical inactivity, obesity may become prevalent, and therefore managing musculoskeletal disorders becomes increasingly important.
- Chuna manual therapy (CMT) is a traditional medicine approach wherein practitioners use their hands or specific tools to provide effective stimulation to address physical issues in the body [4]. Several randomized controlled trials (RCTs) have reported the efficacy of CMT in the treatment of various diseases [5–7]. In Korea, the safety and effectiveness of CMT has been recognized, and as of April 8, 2019, following an amendment by the ordinance of the Ministry of Health and Welfare, CMT has been included in the national health insurance coverage [8].
- Numerous studies on CMT have been conducted, and research in the form of systematic reviews (SRs) on CMT have also increased. Many of these SRs have investigated the effect of CMT on musculoskeletal disorders [9]. Furthermore, SRs on the treatment of conditions/diseases other than musculoskeletal disorders with CMT have also been published, including conditions such as irritable bowel syndrome [10], stroke [11], and primary dysmenorrhea [12].
- Hundreds of thousands of clinical trial studies are published annually [13]. In healthcare, the outcomes of many of these studies are considered for treatment decisions. SRs of individual studies helps assess, summarize, and integrate research. However, in recent years there have been an abundance of reviews, causing redundancy [14,15].
- To address this, umbrella reviews of SRs aim to identify, evaluate, summarize, and compare all relevant reviews, providing clinicians with the important outcomes of SRs synthesized to offer reliable evidence [16].
- Therefore, we conducted an umbrella review of SRs on CMT for musculoskeletal disorders to examine the current state of research on CMT for musculoskeletal disorders and examine the efficacy and safety of CMT for musculoskeletal disorders.
Introduction
- 1. Protocol and registration
- The protocol was developed based on the reporting guidelines provided in the Preferred Reporting Items for Systematic Review and Meta-Analysis statement [17] and has not been published or registered.
- 2. Eligibility criteria
- SRs of RCTs on CMT for musculoskeletal disorders which specified “Chuna,” or “Tuina,” as an intervention were included in this umbrella review. Detailed inclusion and exclusion criteria are shown in Supplementary Material 1.
- 3. Information sources and search strategy
- Searches on SRs published from inception (inception of each database) to August 30, 2023 were performed across nine databases: three databases in English (Cochrane Library, EMBASE, and MEDLINE), one database in Chinese (CNKI), and four databases in Korean (KMBASE, KISS, ScienceOn, and OASIS). In addition, protocols registered on the international database Prospective Register of Systematic Reviews in health and social care were searched.
- The search keywords varied slightly according to the database used but primarily included “Chuna,” “Tuina,” “meta-analysis,” and “systematic review.” The search strategies for English databases are provided in Supplementary Material 2. Korean and Chinese databases were also searched using a similar strategy. All retrieved documents were managed using Endnote 20 software.
- 4. Study selection
- Duplicate documents were initially removed using Endnote 20 software. Then, two reviewers independently conducted an initial screening based on the titles and abstracts. During this screening, any remaining duplicates were manually excluded and the predefined selection (inclusion/exclusion) criteria were fulfilled. Full texts were extracted for all eligible RCTs that met the inclusion/exclusion criteria, and two reviewers assessed eligibility. In cases of disagreement between the two reviewers, a third more senior reviewer made the final decision.
- 5. Data extraction
- Data extraction was carried out by two reviewers and the extracted data was reviewed by a third more senior reviewer. The following data were extracted: year of publication, authors, title, journal, period of running searches, objectives, patients, intervention, comparators, number of studies, total number of patients, outcomes, and main results. Data for outcomes were extracted, focusing on outcome measures of pain, functional outcome measures, and the effective rate. If outcomes other than the above were determined to be important based on patients’ characteristics and conditions, they were also extracted. For outcomes subjected to meta-analysis, statistical significance (significant/not significant) was recorded, along with the results presented using the 95% confidence interval. For outcomes/variables without data synthesis, the number of RCTs reporting significant and non-significant results was recorded separately. In cases where both significant and non-significant results coexisted for a single outcome, it was labeled as “conflicted results.”
- 6. Quality assessment
- A quality assessment was performed for all included SRs, examining the quality of methodology based on A Measurement Tool to Assess Systematic Reviews (AMSTAR) checklist [18]. AMSTAR checklist consists of 11 questions, and each question is answered with options of Yes/No/Can’t answer/Not applicable. Detailed evaluation questions are shown in Supplementary Material 3.
Materials and Methods
- 1. Search results
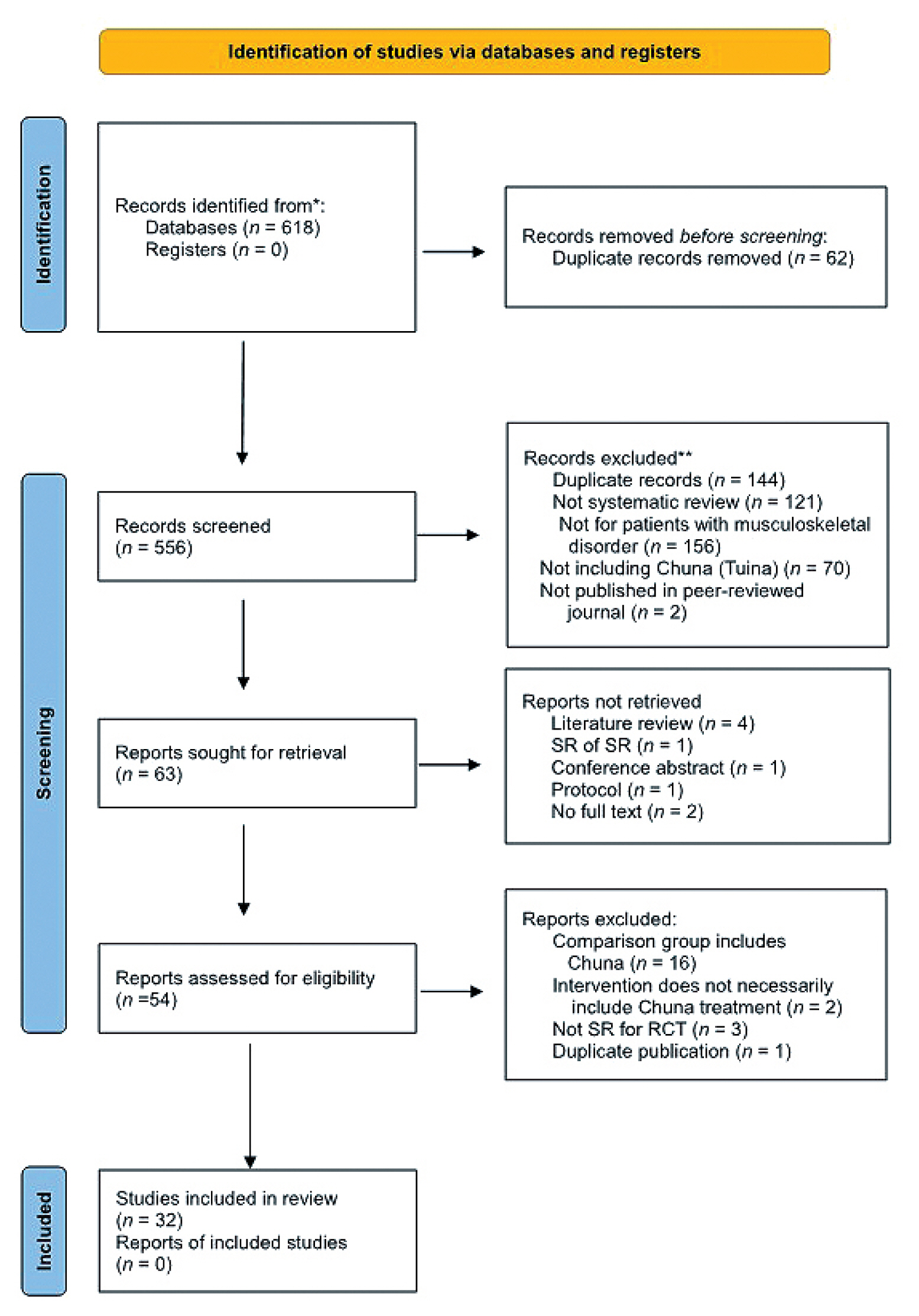
- A flowchart depicting the literature search and study selection process is presented in Fig. 1. There were 618 records retrieved from nine databases, and a total of 32 SRs were included in this umbrella review of SRs (Fig. 1).
- 2. Description of included reviews
- The basic characteristics, interventions, comparisons, and outcomes of the selected SRs are summarized in Table 1. When the musculoskeletal disorder was categorized by the affected region of the body, four SRs focused on cervical disorder, seven SRs focused on thoracolumbar disorder, five SRs focused on upper extremity disorder, nine SRs focused on lower extremity disorder, and eight SRs focused on other types of musculoskeletal disorders.
- On examining the SRs by year of publication, most of the included SRs were published recently, with 15 SRs published from 2021 to 2023 and 10 SRs published from 2018 to 2020. Only one SR was published before 2010, and seven SRs were published from 2010 to 2017.
- Almost all the included SRs included searches of English and Chinese language databases, and if the author was Korean, Korean databases were searched in addition to the English and Chinese databases. Eight SRs performed additional manual searching, such as references, as well as searches across electronic databases. The number of RCTs included in the respective SRs varied widely, from as few as three RCTs to as many as 66 RCTs.
- Eleven SRs aimed to evaluate the efficacy and safety of CMT for specific conditions/diseases and symptoms of musculoskeletal disorders, and in the case of the other 21 SRs, only efficacy was mentioned as the objective of the SR.
- As for the interventions described in the selected SRs, there were those with CMT alone or a combined therapy of CMT and other treatments including acupuncture, functional exercise therapy, topical herbal preparations, intra articular injections of sodium hyaluronate (Table 1). As the comparison interventions there were treatments including acupuncture, traction, sham treatment, functional exercise therapy, intra articular injections of sodium hyaluronate, use of nonsteroidal anti-inflammatory drugs, use of traditional and Western medicine and treatments other than CMT (Table 1).
- The outcomes extracted from most of the included SRs were outcome measures of pain (n = 27), effective rate (n = 22), and functional outcome measures (n = 15). In addition, depending on the characteristics of the musculoskeletal disorder, SRs used a duration of morning stiffness, blood flow velocity, Harris hip score, deep vein thrombosis incidence rate, and the Fibromyalgia Impact Questionnaire as outcomes (Table 1).
- In all included SRs, a risk of bias assessment was conducted for the RCTs included in each SR (except for two SRs [19,20]). As a result of the risk of bias evaluation, except for one SR that did not use the Cochrane tool where all seven included RCTs were evaluated as fair, all other SRs showed that the risk of bias of the included RCTs was high or unclear.
- 3. Quality of included SRs
- The results of quality assessment using AMSTAR are outlined in Supplementary 4. Except for three SRs with “high” quality and two SRs with “low” quality, all the other included SRs were assessed to be “medium” quality.
- 4. Main results
- The main results of the SRs included in this umbrella review are summarized in Table 2. Effective rate was reported in 23 SRs, of which 19 SRs included meta-analysis, and 17 SRs reported that CMT showed a significant difference in terms of the effective rate. Pain outcome measures were reported in 20 SRs, wherein 16 SRs conducted meta-analyses, of which 12 SRs reported that CMT showed a significant difference in terms of pain outcomes. Functional outcome measures were reported in 12 SRs, wherein 8 SRs conducted meta-analysis, of which one SR reported no significant difference depending on the type of outcome measures, but all the other SRs showed a significant difference in terms of functional outcomes.
- 5. Adverse events
- A total of 20 SRs reported on adverse events (AEs). Among these SRs, six stated that none of the included RCTs reported AEs. Four SRs reported no AEs from all RCTs that included AE data. Two SRs provided specific information on the type of AEs (skin redness, an increase in discomfort). In one SR, a meta-analysis was conducted on AEs, and reported that CMT was safer than surgical treatment [RR 0.45 (0.26, 0.76)]. Among the reported AEs, no serious AEs were observed.
Results
2.1. General characteristics
2.2. Aims
2.3. Intervention and comparisons
2.4. Outcome measures
2.5. Risk of bias of included trials
- In Korea, there is a growing interest in CMT due to its inclusion in national health insurance coverage, leading to an increase in the number of clinical trials and systematic literature research on CMT. Therefore, in this study, we synthesized the important outcomes of SRs on CMT used for the treatment of musculoskeletal disorders to provide a better understanding and establish reliable evidence for the efficacy and safety of CMT.
- The search yielded a total of 32 SRs. These articles covered a wide range of musculoskeletal areas, including cervical, thoracolumbar, upper extremity, and lower extremity regions. As for the type of specific conditions of musculoskeletal disorders, SRs on knee osteoarthritis accounted for the largest number (n = 6), followed by LBP (n = 3), temporomandibular disorders (n = 3), musculoskeletal pain (n = 2), and cervical disc herniation (n = 2). Of the 32 SRs, 25 SRs were published within the past five years, indicating that SRs on CMT have been conducted relatively recently.
- In most of the SRs included in this umbrella review, CMT alone or a combination therapy with CMT was used as the intervention, and treatments other than CMT were used as comparison treatments without adding other conditions or restrictions. Outcomes were extracted, centered on pain outcome measures, effective rate, and functional outcome measures, and depending on the characteristics of different types of musculoskeletal disorders, other specific outcomes such as deep vein thrombosis incidence were added.
- Summarizing the main results of the SRs included in this review, CMT showed significantly better outcomes of improvement over comparisons in terms of effective rate (17/19 SRs), pain outcome measures (12/16 SRs), and functional outcome measures (8/12 SRs). These findings suggest that CMT can serve as an effective treatment method for various types of musculoskeletal disorders.
- As for safety, 20 of 32 SRs reported on AEs, of which six SRs stated that no RCTs reported the occurrence of AEs. In addition, all the reported AEs were mild in severity, such as skin redness. Thus, CMT is a relatively safe mode of treatment. However, since many of the RCTs included in SRs did not present a report on AEs, and even when they did, the information given did not provide enough details. Therefore, it is reasoned that more RCTs and SRs need to be conducted with safety assessments.
- This umbrella review only examined SRs of RCTs on musculoskeletal disorder, however, Chuna is used for a variety of conditions/diseases. Therefore in the future, the SRs for non-musculoskeletal conditions/diseases which included insomnia [52,53], nocturnal enuresis, functional dyspepsia [54], anorexia, allergic rhinitis, constipation [55,56], headache [57–59], irritable bowel syndrome [60,61], fatigue [62], hypertension [63,64], and dysmenorrhea [65] excluded during screening in this review can be reviewed. The various techniques of Chuna increase its applicability [66].
- Several factors need to be considered when interpreting the findings of this umbrella review. Firstly, the definition of CMT has not been fully established. In Korea, CMT is based on manual therapy that addresses biomechanical function, diagnostics, pathology, and theories related to treatment to achieve balance in the orthopedic structures and functions [4] in the musculoskeletal system. Representative techniques of CMT include thrust, mobilization, distraction of the spine and joints, soft tissue release, visceral manipulation, and craniosacral therapy [67]. However, the definition and scope of these Korean “Chuna” or Chinese “Tuina” manual therapies have not been clearly established, and interpretation may differ depending on the perspectives of the clinicians or researchers. Secondly, the overall quality of the SRs included in this study was low, indicating a risk of bias. When the quality assessment was conducted using AMSTAR checklist, only 3 of the 32 SRs were rated as “high.” Additionally, 18 of the SRs failed to meet more than half of the assessment criteria (out of a total of 11 items). Most of the included SRs did not have a predetermined design, did not disclose conflicts of interest, did not search for literature outside of traditional publishing, and did not provide a list of excluded studies. Furthermore, in this umbrella review, such literature was excluded, and we did not manually search for journals that were not included in the databases or references of the included this type of literature. Therefore, some SRs may have been inadvertently omitted from this umbrella review. Furthermore, in most cases, only one SR was included for each type of musculoskeletal disorder, such as knee osteoarthritis, temporomandibular disorders, and cervical disc herniation. This means that many other types of musculoskeletal disorders and affected areas were not covered in the SRs included in this study. To arrive at a conclusion with high-quality evidence for each type of musculoskeletal disorder, more RCTs and SRs that synthesize the RCTs should be conducted. Despite these limitations, in umbrella review of SRs, we conducted a literature search in English, Chinese, and Korean databases to minimize the omission of studies. This review encompassed a wide range of musculoskeletal disorders, leading to a more comprehensive understanding of the RCTs on CMT for musculoskeletal disorders and its reported effectiveness outcomes. The findings of this review are expected to provide valuable information for clinicians utilizing CMT in their practice, researchers planning and designing RCTs on CMT, and patients with musculoskeletal disorders exploring different treatment options.
Discussion
- CMT appears to be a safe and effective treatment option for a wide range of musculoskeletal conditions. However, the limited number of studies and the generally low quality of included SRs should be considered when interpreting these results.
Conclusion
Supplementary Material
-
Author Contributions
Conceptualization: BCS. Methodology: DK. Formal analysis: GB. Investigation: DK. Writing original draft: DK and GB. Writing - review and editing: BCS.
-
Conflicts of Interest
None.
-
Funding
None.
-
Ethical Statement
This research did not involve any human or animal experiments.
Article information
Data Availability
| Author, y [ref.] | Aims | Time period of search and databases used for search | No. included RCTs (patients) | Patients | Interventions | Comparisons | Outcomes |
|---|---|---|---|---|---|---|---|
| Cervical (n = 4) | |||||||
| Wang et al, 2008 [19] | Evaluation of the efficacy of CMT for treatment of symptoms of cervical spondylosis | 1996–2007; 6 E and 2 Ch DB | 7 (926) | Cervical spondylosis | CMT alone | Treatment other than CMT |
1) Blood flow velocity 2) Blood viscosity 3) Severity of headache and vertigo |
| Zhou et al, 2016 [21] | Evaluation of the efficacy and safety of a combined therapy of CMT + acupuncture for the treatment of cervical disc herniation | Time period not specified; 2 Ch and 2 E DB + manual-searching | 5 (347) | Cervical disc herniation | CMT + acupuncture | Acupuncture | 1) Effective rate |
| Yang et al, 2013 [22] | Comparative evaluation of the efficacy and safety of CMT VS traction for the treatment of cervical disc herniation | Up to April 16, 2013; 3 Ch and 2 E DB | 30 (2,807) | Cervical disc herniation | CMT alone | Traction |
1) Effective rate 2) Pain outcome |
| Lee et al, 2016 [23] | Evaluation of the effects of CMT on cervical pain | Up to July 2016; 2 K, 4 E, and 1 Ch DB | 7 (571) | Cervical pain | CMT alone | Treatment other than CMT |
1) Pain outcome (NRS, VAS) 2) Functional outcome (NDI) |
|
|
|||||||
| Thoracolumbar (n = 7) | |||||||
|
|
|||||||
| Zhou et al, 2023 [24] | Evaluation of the therapeutic effects of CMT on chronic/non-acute LBP | Up to May 2022; 3 E and 4 Ch DB | 17 (1,628) | LBP | CMT (alone or combined) | Usual care, sham Tuina/placebo, no treatment/wait list |
Not performed data synthesis and results analysis. RCTs included pain intensity, physical disability |
| Yang et al, 2023 [25] | Evaluation of the treatment effects and safety of CMT on chronic/nonspecific LBP | Up to December 30, 2019; 7 E and 5 Ch DB + manual-searching | 15 (1,390) | LBP | CMT (alone or combined) | Treatment other than CMT |
1) Pain outcome 2) Functional outcome 3) Quality of life measures |
| Cho et al, 2021 [26] | Evaluation of the effects of CMT on postpartum LBP | Up to September 2021; 6 K, 5 E, and 1 Ch DB | 4 (454) | LBP | CMT (alone or combined) | Treatment other than CMT |
Not performed data synthesis 1) Pain outcome (VAS) 2) functional outcome (ODI) 3) Effective rate |
| Wang et al, 2022 [27] | Presenting evidence for effects of CMT + acupuncture for treatment of LDH | January 2012 – December 2020; 4 Ch DB + manual-searching | 15 (1,786) | LDH | CMT + acupuncture | Acupuncture | 1) Effective rate |
| Rao et al, 2019 [28] | Efficacy and safety of CMT for acute lumbar sprain | Up to October 2018; 4 Ch and 2 E DB | 11 (851) | Acute lumbar sprain | CMT (alone or combined) | Treatment other than CMT |
1) Efficacy rate 2) Pain outcome (VAS) 3) Recovery rate |
| Hong et al, 2020 [29] | Evaluation of the effect of CMT on spondylolisthesis | Up to August 2020; 4 K, 5 E and 1 Ch DB | 11 (910) | Spondylolisthesis | CMT (alone or combined) | Treatment other than CMT |
1) Effective rate 2) Pain outcome (VAS) |
| Lim et al, 2018 [30] | Evaluation of efficacy and safety of CMT for lumbar spinal stenosis | Up to October 2018; 6 K, 3 E and 1 Ch DB + manual-searching | 3 (220) | Spinal stenosis | CMT (alone or combined) | Treatment other than CMT |
1) pain outcome (VAS) 2) effective rate |
|
|
|||||||
| Upper extremity (n = 5) | |||||||
|
|
|||||||
| Yan et al, 2021 [31] | Systematic review of efficacy of CMT for treatment of shoulder pain | Up to December 2019; 3 E and 2 Ch DB | 11 (1,100) | Shoulder pain | CMT (alone or combined) | Treatment other than CMT |
1) Pain outcome 2) Functional outcome (ROM) 3) Muscle strength assessment |
| Hong et al, 2021 [32] | Evaluation of efficacy of CMT for treatment of rotator cuff disorder | Up to January 2022; 4 K, 2 E and 2 Ch DB | 4 (284) | Rotator cuff disorder | CMT (alone or combined) | Treatment other than CMT |
Not performed data synthesis. 1) Pain outcome 2) Effective rate |
| Cho et al, 2019 [33] | Evaluation of the effects of CMT on treatment of adhesive capsulitis | Up to August 2019; 5 K, 4 E and 1 Ch DB | 21 (3,016) | Adhesive capsulitis | CMT (alone or combined) | Treatment other than CMT |
1) Pain outcome (VAS, NRS) 2) Effective rate |
| Han et al, 2022 [34] | Evaluation of the treatment effect of CMT for lateral epicondylitis of humerus | Up to April 2022; 5 K, 3 E, 1 Japanese, and 1 Ch DB | 8 (675) | Lateral epicondylitis of humerus | CMT (alone or combined) | Treatment other than CMT |
Not performed data synthesis 1) Effective rate 2) Pain outcome (VAS) 3) Ability of daily life |
| Park et al, 2021 [35] | Evaluation of efficacy and safety of CMT for carpal tunnel syndrome | Up to October 2021; 6 K, 4 E and 2 Ch DB + manual searching | 504 | Carpal tunnel syndrome | CMT (alone or combined) | Treatment other than CMT |
1) Effective rate 2) Pain outcome (VAS) 3) Functional outcome (BCTQ) |
|
|
|||||||
| Lower extremity (n = 9) | |||||||
|
|
|||||||
| Lee et al, 2022 [36] | Evaluation of effect of CMT for management of symptoms after hip replacement surgery | Up to January 2022; 5 K, 2 E and 2 Ch DB | 11 (410) | Surgery for hip joint | CMT (alone or combined) | Treatment other than CMT |
1) Harris hip score 2) DVT incidence |
| Zang et al, 2023 [37] | Evaluation of effectiveness and safety of CMT for knee osteoarthritis (KOA) | Up to December 2019; 1 E and 4 Ch DB | 6 (359) | Knee osteoarthritis | CMT alone or combination with functional exercise therapy | Blank control, Sham therapy, functional exercise |
1) Pain outcome (VAS) 2) Functional outcome (WOMAC) 3) Walking time |
| Pan et al, 2022 [38] | Systematic review on the reliability of CMT for treatment of KOA | Time period not defined; 5 E and 4 Ch DB | 16 (1,670) | Knee osteoarthritis | CMT (alone or combined) | Treatment other than CMT |
1) Effective rate 2) Pain outcome (VAS) 3) Functional outcome (WOMAC) |
| Liu et al, 2021 [39] | Evaluation of efficacy of a combined therapy of CMT + intra-articular injection of sodium hyaluronate for knee osteoarthritis (KOA) | From January 2001 to December 2019; 1 E and 3 Ch DB, +American medica abstracts DB | 10 (1,016) | Knee osteoarthritis | CMT + Intra-articular injection of sodium hyaluronate | Intra-articular injection of sodium hyaluronate | 1) Effective rate |
| Xu et al, 2019 [40] | Evaluation of effectiveness and safety of CMT for KOA | Up to February 1, 2019; 3 E and 3 Ch DB | 17 (1,387) | Knee osteoarthritis | CMT alone | Treatment other than CMT |
1) Effective rate 2) Pain outcome (VAS) 3) Functional outcome (WOMAC) |
| Chen et al, 2019 [41] | Evaluation of efficacy and safety of CMT monotherapy for KOA | Up to May 2018; 2 E and 3 Ch DB+ manual-searching | 8 (632) | Knee osteoarthritis | CMT alone | Treatment other than CMT |
1) Effective rate 2) Pain outcome (VAS) 3) Functional outcome (JOA) |
| Bai et al, 2018 [42] | Evaluation on the efficacy of a combined therapy (CMT + topical herbal medicine preparations from traditional Chinese medicine) for KOA | Up to November 27, 2017; 1 E and 3 Ch DB | 6 (495) | Knee osteoarthritis | CMT + topical herbal medicine preparations | Oral administration or topical application of NSAIDS |
1) Effective rate 2) Pain outcome 3) Functional outcome |
| Lee et al, 2021 [43] | Evaluation of the effects of CMT for patients undergoing total knee arthroplasty | Up to January 2021; 5 K, 2 E and 2 Ch DB DB | 23 (1,792) | Surgery for knee (total knee arthroplasty) | CMT (alone or combined) | Treatment other than CMT |
1) Effective rate 2) DVT incidence 3) Hospital for special surgery score (HSS) 4) Pain outcome (VAS) 5) Functional outcome (WOMAC) |
| Kwark et al, 2018 [44] | Evaluation of the effects of CMT for ankle sprain | Up to October 2017; 2 K, 3 E, and 1 Ch DB | 24 (1,960) | Ankle sprain | CMT (alone or combined) | Treatment other than CMT |
Not performed data synthesis 1) Pain outcome (VAS, NRS) 2) Functional outcome (AOFAS) 3) Effective rate |
|
|
|||||||
| Others (n = 8) | |||||||
|
|
|||||||
| Moon et al, 2012 [45] | Evaluation of CMT efficacy for musculoskeletal pain reported in Korean literature | Up to April 2011; 7 K DB + manual-searching | 6 (207)* | Musculoskeletal | CMT (alone or combined) | Treatment other than CMT |
Not performed data synthesis Efficacy of experimental group (Positive significant effect / not significant different / negative significant effect) |
| Lee et al, 2017 [46] | Systematic review of the effects of CMT on the outcomes of pain and function for patients with musculoskeletal disorders | Up to December 2016; 3 Ch, 1 Japanese, and 7 K DB + manual-searching | 66 (6,170)† | Musculoskeletal | CMT (alone or combined) | Treatment other than CMT |
1) Pain outcome (VAS, NRS) 2) Functional outcome (NDI, ODI) |
| Lee et al, 2023 [47] | Evaluation of the effects of CMT on TMD | Up to March 2020; 4 E, 1 Ch, 1 Japanese, and 5 K DB | 12 (863) | TMD (aged 19 years or older) | CMT (alone or combined) | usual care |
1) Effective rate 2) Pain outcome 3) Functional outcome |
| Bae et al, 2017 [48] | Evaluation on the effects of CMT for treatment of TMD | Up to May 2017; 6 K, 3 E, and 1 Ch DB | 14 (989) | TMD | CMT (alone or combined) | Treatment other than CMT |
1) Effective rate, 2) Pain outcome (VAS) |
| He et al, 2023 [49] | Systematic review on the efficacy and safety of CMT on TMD | Up to July 2022; 3 E and 3 Ch DB | 13 (1,141) | TMD | CMT (alone or combined) | Treatment other than CMT |
1) Effective rate 2) Pain outcome (degree of pain relief) 3) Maximum active opining degree 4) Friction index |
| Kim et al, 2018 [50] | Evaluation on the effects and safety of traditional Chinese medicine including CMT for treatment of osteoarthritis | Up to May 2018; 3 K, 4 E, and 1 Ch DB | 7 (633) | Osteoarthritis | CMT (combined) | Treatment other than CMT |
1) Effective rate 2) Pain outcome (VAS) 3) Functional outcome (JOA) |
| Heo et al, 2018 [51] | Evaluation on the effects of CMT for treatment of rheumatoid arthritis | Up to April 2018; 4 K, 4 E, and 1 Ch DB | 5 (314) | Rheumatoid Arthritis | CMT (combined) | Usual care of traditional Korean medicine, medications of conventional medicine |
1) Effective rate 2) Pain outcome (VAS) 3) Duration of morning stiffness |
* TMD 2/neck pain 2/LBP 2.
† Cervical 24, Thoracolumbar 14, Upper extremity 13, Lower extremity 10, Others 4.
AOFAS = American Orthopedic Foot and Ankle Society; BCTQ = Boston Carpal Tunnel Questionnaire; Ch = Chinese; DB = databases; DVT = deep vein thrombosis; E = English; FIQ = Fibromyalgia Impact Questionnaire; HSS = Hospital for Special Surgery Knee-Rating Scale; JOA = Japanese Orthopedic Association; K = Korean; NDI = neck disability index; NRS = numeric rating scale; ROM = range of motion; VAS = visual analog scale; WOMAC = The Western Ontario and McMaster Universities Osteoarthritis Index.
| Author, y [ref.] | Effective rate | Pain outcome | Functional outcome | Other outcomes | AE |
|---|---|---|---|---|---|
| Cervical | |||||
|
|
|||||
| Wang et al, 2008 [19] |
Blood flow velocity (980 patients): not significant - Hedgee’s g: 0.25 (−0.02 to 0.51) Vertigo and headache (data not synthesized): not significant |
||||
| Zhou et al, 2016 [21] |
Significant (n = 5): OR 2.87 [1.30, 6.30] |
1) Recovery rate: significant OR 1.97 [1.28, 3.03] |
AEs reported in no RCTs | ||
| Yang et al, 2013 [22] |
Significant (n = 22) RR 3.13 [2.27, 4.32] |
Significant (n = 9) MD −1.20 [−1.39, −1.02], |
AEs were reported in 14 RCTs. -no AE (n = 8) -mild AE (n = 6) |
||
| Lee et al, 2016 [23] |
Significant -CMT vs traction (n = 5): SMD −1.01 [−1.67, −0.34], -CMT vs medication (n = 2): SMD −0.62 [−1.03, −0.21], |
Significant -CMT vs traction (n = 1) MD −3.60 [−6.67, −0.53], |
|||
|
|
|||||
| Thoracolumbar | |||||
|
|
|||||
| Zhou et al, 2023 [24] | No discussion on the outcomes | ||||
| Yang et al, 2023 [25] |
Significant (n = 12) SMD −0.82 [−1.12, −0.53] |
Significant (n = 2) SMD −0.91 [−1.55, −0.27] |
1) Quality of life (n = 2): not significant SMD 0.58 [−0.04, 1.21] |
AEs were reported in 6 RCTs. -No SAE: n = 6 |
|
| Cho et al, 2021 [26] |
Data not synthesized (n = 4) conflicted results −2 RCTs Significant, 2 RCTs not significant |
Data not synthesized (n = 2) - significant in all 2 RCTs |
Data not synthesized (n = 1) - significant in all 1 RCT |
No specific reports on AEs | |
| Wang et al, 2022 [27] |
Significant (n = 15) OR 4.59 [3.15, 6.69] |
||||
| Rao et al, 2019 [28] |
Significant (n = 11) OR 5.47 [3.27, 9.16] |
Significant (n = 4) WMD −2.24 [−2.36, −2.21] |
1) Recovery rate: significant (n = 11) OR 3.78 [2.34, 6.11] |
AEs were reported in 1 RCT. -No SAE: n = 1 |
|
| Hong et al, 2020 [29] |
Significant -CMT vs traction (n = 3): RR 7.36 [2.96, 18.29], -CMT + exercise vs traction + exercise (n = 3) RR 2.83 [1.39, 5.75] |
AEs were reported in 2 RCTs -no ae: n = 2 |
|||
| Lim et al, 2018 [30] |
Significant (n = 3) -RR 1.32 [1.11, 1.57] |
AEs were reported in 1 RCT | |||
|
|
|||||
| Upper extremity | |||||
|
|
|||||
| Yan et al, 2021 [31] |
Significant (n = 8) SMD −1.15 [−1.76, −0.54] |
Significant (n = 8) WMD −9.71 [−10.36, −9.07] |
1) Muscle strength assessment (n = 7): significant WMD −0.02 [−0.29, −0.1] 2) Daily living skills assessment (n = 7): significant WMD −2.37 [−2.72, −2.02], |
||
| Hong et al, 2021 [32] |
Data not synthesized. Conflicted results (n = 2) −1 significant, 1 not significant |
Data not synthesized. Conflicted results (n = 3) −2 significant, 1 not significant |
AEs were reported in 2 RCTs. -no ae: n = 1 -feeling of stiffness: n = 1 |
||
| Cho et al, 2019 [33] |
Significant -CMT vs Acu (n = 10): RR 1.10 [1.02, 1.18] -CMT + Acu vs Acu (n = 12): RR 1.19 [1.14, 1.23] |
Significant -CMT vs Acu (n = 4): SMD −0.45 [−1.06, 0.17] -CMT + Acu vs Acu (n = 2): SMD −1.81 [−2.54, −1.08], |
|||
| Han et al, 2022 [34] |
Data not synthesized (n = 7) - significant in all 7 RCTs |
Data not synthesized (n = 4) - significant in all 4 RCTs |
Data not synthesized (n = 5) - significant in all 5 RCTs |
AEs were reported in 2 RCTs -mild skin redness: n = 2 |
|
| Park et al, 2021 [35] |
Significant -CMT + KM vs WM (n = 2): RR 1.69 [1.35, 2.13], -CMT + KM vs WM (n = 4): RR 1.38 [1.14, 1.65] |
||||
|
|
|||||
| Lower extremity | |||||
|
|
|||||
| Lee et al, 2022 [36] |
1) Harris hip score: significant -CMT + UC vs UC (n = 2): MD 9.55 [7.18, 11.91] -CMT + fumigation therapy vs UC (n = 2): MD 2.91 [2.33, 3.50] 2) Incidence of DVT: conflicted results -CMT + UC vs UC (n = 4): Significant RR 0.25 [0.12, 0.52] -CMT + herbal medicine vs UC (n = 2): not significant RR 0.55 [0.21, 1.40], p=0.21 |
||||
| Zang et al, 2023 [37] |
Not significant (n = 6) MD −0.38 [−1.35, −0.19] |
1) Walking time (n = 2): significant MD −1.60 [−2.57, −0.63] |
AEs were reported in 1 RCT -an increase in discomfort: n = 1 |
||
| Pan et al, 2022 [38] |
Significant (n = 13) OR 4.53 [3.06, 6.69] |
Significant (n = 13) MD −2.72 [−4.19, −1.25] |
Significant (n = 6) MD −14.21 [−14.86, −13.56] |
HS score (n = 2): significant MD 6.32 [4.58, 8.06] |
|
| Liu et al, 2021 [39] |
Significant (n = 10) OR 4.91 [3.05, 7.91] |
||||
| Xu et al, 2019 [40] |
Significant (n = 16) MD 2.30 [1.65, 3.22], |
Not significant (n = 5) |
Significant (n = 5) MD −9.04 [−16.71, −1.36] |
AEs were reported in 3 RCTs -No significant differences between the two groups |
|
| Chen et al, 2019 [41] |
Significant (n = 8) OR 2.03 [1.43, 2.88] |
Significant (n = 2) OR 0.58 [0.22, 0.93] |
Significant (n = 2) OR 0.65 [0.29, 1.01] |
No reports of SAEs | |
| Bai et al, 2018 [42] |
Significant (n = 6) RR 1.20 [1.06, 1.36] |
||||
| Lee et al, 2021 [43] |
Significant -CMT + UC vs UC (n = 2): RR 1.24 [1.10, 1.39] |
Significant -CMT + other therapy vs UC (n = 2): MD −1.44 [−1.81, −1.06] |
Data not synthesized (n = 2) - significant in all 2 RCTs |
1) DVT incidence: significant −CMT + UC vs UC (n = 3): RR −0.16 [−0.25, −0.07] 2) HSS: Significant -CMT + UC vs UC (n = 5): MD 8.89 [5.89, 11.88], -CMT + acupuncture, UC vs UC (n = 4): MD 5.78 [3.56, 8.00], -CMT + herbal medicine, UC vs UC (n = 4): MD 15.27 [6.21, 24.33], |
AEs were reported in 3 RCTs |
| Kwark et al, 2018 [44] |
Data not synthesized (n = 13) conflicted results: −11 significant |
Data not synthesized (n = 10) conflicted results: −6 significant |
Data not synthesized (n = 4) - significant in all 4 RCTs |
No included RCTs reported on AEs | |
|
|
|||||
| Others | |||||
|
|
|||||
| Moon et al, 2012 [45] |
Data not synthesized. conflicted results −3 RCT (1 neck pain, 2 LBP): significant −3 RCT (1 neck pain, 2 TMD): not significant |
No included RCTs reported on AEs | |||
| Lee et al, 2017 [46] |
Significant -CMT vs sham (n = 1): SMD −3.09 [−3.59, −2.59], -CMT vs traction (n = 9): SMD −0.64 [−0.87, −0.40], -CMT vs physical therapy (n = 3): WMD−0.97 [−1.46, −0.48], -CMT vs drug (n = 5): WMD −0.44 [−0.85, −0.02] |
NDI (n = 3): not significant SMD −1.45 [−2.92, 0.02] ODI: significant SMD −1.79 [−3.54, −0.04] shoulder function (n = 2): not significant WMD 3.33 [−4.59, 11.25], |
Reported in 7 RCTs -CMT was superior when compared with surgery (n = 5) RR 0.45 [0.26, 0.76] |
||
| Lee et al, 2023 [47] |
Significant -CMT vs US (n = 3): RR 1.15 [1.05, 1.27] -CMT + TCM vs TCM (n = 4): RR 1.21 [1.10, 1.32], -CMT + UC vs UC (n = 2): RR 1.28 [1.08, 1.52] |
Significant -CMT vs UC (n = 3): MD −1.17 [−1.71, −0.64] -CMT + TCM vs TCM (n = 2): MD 0.24 [0.12, 0.35] |
Reported in 3 RCTs -no AE: n = 3 |
||
| Bae et al, 2017 [48] |
Conflicted results -CMT + E.acu vs E.acu (n = 2): significant RR 0.16 [0.06, 0.27], -CMT vs acu (n = 2): not significant RR 1.09 [0.98, 1.20] -CMT vs DHT (n = 2): significant RR 1.16 [1.02, 1.31], |
No RCTs reported on AEs | |||
| He et al, 2023 [49] |
Significant (n = 12) -RR 1.21 [1.16, 1.27], |
Significant (n = 5) -MD −0.91 [−1.39, −0.42] |
1) Maximum active opining degree (n = 2): significant -MD 4.88 [3.20, 6.56], 2) Friction index (n = 4): significant -DI index: MD −0.07 [−0.11, −0.02] -PI index: MD −0.04 [−0.07, −0.00] |
No report on AEs in both groups | |
| Kim et al, 2018 [50] |
Significant (n = 6) -RR 1.21 [1.13, 1.30] |
Significant (n = 2) SMD 0.92 [0.15, 1.70], |
Significant (n = 3) -RR 1.89 [1.55, 2.24] |
No RCTs reported on AEs | |
| Heo et al, 2018 [51] |
Conflicted results -CMT + KM vs medication (n = 4): significant RR 1.50 [1.28, 1.75], -CMT + medication vs medication (n = 1): not significant RR 1.19 [1.00, 1.42] |
Significant -CMT + KM vs medication (n = 3): SMD −2.55 [−2.98, −2.11] |
Duration of morning stiffness: significant -CMT + KM vs medication (n = 3): SMD −0.63 [−0.98, −0.28] |
||
All values are presented with 95% confidence intervals.
Acu = acupuncture; AE = adverse events; CMT = Chuna manual therapy; DHT = deep heat therapy; E.acu = electro acupuncture; KM = Korean medicine; MD = mean difference; OR = Odds ratio; RR = relative ratio; SAE = serious adverse event; SMD = standardized mean difference; UC = usual care; WM = western medicine; WMD = weight mean difference.
(n = number of RCTs included in each SR).
- [1] Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ 2003;81(9):646−56.PubMedPMC
- [2] Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2021;396(10267):2006−17.ArticlePubMed
- [3] Word Health Organization [Internet]. Musculoskeletal health: 2022 [cited 2023 August 29]. Available from: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions
- [4] Park T-Y, Moon T-W, Cho D-C, Lee J-H, Ko Y-S, Hwang E-H, et al. An introduction to Chuna manual medicine in Korea: History, insurance coverage, education, and clinical research in Korean literature. Integr Med Res 2014;3(2):49−59.ArticlePubMedPMC
- [5] Chen MY, Pu QQ, Liu SY, Jiang ZY. Efficacy comparison of different stimulation therapies for periarthritis of shoulder. Zhongguo Zhen Jiu 2013;33(2):109−12. [in Chinese].PubMed
- [6] Lu M, Liu X. Insomnia due to deficiency of both the heart and spleen treated by acupuncture-moxibustion and Chinese tuina. J Tradit Chin Med 2008;28(1):10−2.ArticlePubMed
- [7] PLaZS Qi. To observe the curative effect of Tongyang Sanjie massage method in the treatment of coronary heart disease with stable angina pectoris. Chinese Community Doctors 2014;30(13):79−80. https://caod.oriprobe.com/articles/42017119/To_observe_the_curative_effect_of_Tongyang_Sanjie_massage_method_in_th.htm.
- [8] Park JS, Lim HH. Analysis of Chuna Manual Therapy Usage Status after the Application of Chuna Manual Therapy Health Insurance 2019–2021. J Korean Rehabil Med 2022;32(4):61−72. [in Korean].Article
- [9] Kim HK, Gwon TU, Kim BJ. Chinese Medicine including Chuna Manual Therapy for Osteoarthritis : A Systematic Review. J Chuna Man Med Spine Nerves 2018;13(1):11−21.Article
- [10] Bu FL, Han M, Lu CL, Liu XH, Wang WG, Lai JL, et al. A systematic review of Tuina for irritable bowel syndrome: Recommendations for future trials. Complement Ther Med 2020;52:102504. ArticlePubMed
- [11] Han MKC. Chuna Manual Therapy for Stroke: A Systematic Review and Meta-analysis. J Chuna Man Med Spine Nerves 2019;14(2):15−28.Article
- [12] Lv Y, Feng H, Jing F, Ren Y, Zhuang Q, Rong J, et al. A systematic review of Tuina for women with primary dysmenorrhea: A protocol for systematic review and meta-analysis. Medicine (Baltimore) 2021;100(47):e27935. PubMedPMC
- [13] Ghersi D, Pang T. From Mexico to Mali: four years in the history of clinical trial registration. J Evid Based Med 2009;2(1):1−7.ArticlePubMed
- [14] Bastian H, Glasziou P, Chalmers I. Seventy-five trials and eleven systematic reviews a day: how will we ever keep up? PLoS Med 2010;7(9):e1000326. ArticlePubMedPMC
- [15] Moher D, Tetzlaff J, Tricco AC, Sampson M, Altman DG. Epidemiology and reporting characteristics of systematic reviews. PLoS Med 2007;4(3):e78. ArticlePubMedPMC
- [16] Smith V, Devane D, Begley CM, Clarke M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med Res Methodol 2011;11(1):15. ArticlePubMedPMCPDF
- [17] Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 2009;151(4):264−9. W64. ArticlePubMed
- [18] Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N, Hamel C, et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. Methodol 2007;7:10. ArticlePubMedPMCPDF
- [19] Wang MY, Tsai PS, Lee PH, Chang WY, Yang CM. Systematic review and meta-analysis of the efficacy of tuina for cervical spondylosis. J Clin Nurs 2008;17(19):2531−8.ArticlePubMed
- [20] Yan Z, Ma Z, Ma X, Kong L, Yan J. Meta-analysis of the efficacy of Tuina in the treatment of shoulder pain. Shanghai Med Pharma J 2021;42(15):36−9. http://open.oriprobe.com/articles/61724938/Meta_analysis_of_the_efficacy_of_Tuina_in_the_trea.htm.
- [21] Fanyuan Z, Fushui L, Xiang W, Meimei Z. Meta-analysis of acupuncture combined with tuina treatment of cervical spondylotic radiculopathy. Tradit Chin Med J 2016;15(2):37−9.
- [22] Xin-jun YJZR-cW. Meta-analysis on nerve-root-type cervical spondylosis treatment by manipulation and cervical traction. Glob Tradit Chin Med 2013;6(9):641−8.
- [23] Lee K, Ha I, Kim H, Bae Y, Kim N, Suh C, et al. Chuna Manual Therapy for Neck Pain : A Systematic Review and Meta-analysis. J Chuna Man Med Spine Nerves 2016;11(2):11−21. https://www.chuna.or.kr/board/file/201612/JKCMSN2016;11(2)%2011-21.pdf.
- [24] Zhou X, Ma Q, Yang J, Mohabbat AB, Croghan IT, la Choo Tan C, et al. Clinical outcome measures reporting in randomized trials evaluating Tuina therapy for chronic nonspecific low back pain: A systematic review. Medicine (Baltimore) 2023;102(16):e33628. ArticlePubMedPMC
- [25] Yang J, Zhou X, Ma Q, Woods JT, Mohabbat AB, Do A, et al. Efficacy and safety of Tuina for chronic nonspecific low back pain: A PRISMA-compliant systematic review and meta-analysis. Medicine (Baltimore) 2023;102(9):e33018. ArticlePubMedPMC
- [26] Cho J, Park I-, Hwang M, Heo I. Chuna Manual Therapy for Postpartum Low Back Pain: Systematic Review. J Chuna Man Med Spine Nerves 2021;16(2):1−8.Article
- [27] Zhiwen W, Lun H, Shuang H, Yangchun L, Yijiao S, Sen R. Meta-analysis of Acupuncture Combined With Massage in Treating Lumbar Disc Herniation. China Health Standard Manag 2022;13(19):147−51.
- [28] Zilong R, Anting L, Nanchang S. Systematic review on TUINA for treatment of acute lumbar sprain. J Tradit Chin Orthop Trauma 2019;31(12):29−33.
- [29] Hong S, Ha H, Yoon K. Chuna Manual Therapy for Spondylolisthesis: A Systematic Review and Meta-analysis. J Korean Med Rehabil 2020;30(4):65−77.Article
- [30] Lim K, Shin B, Heo I, Hwang M. Chuna Manual Therapy for Lumbar Spinal stenosis: A Systematic Review. J Chuna Man Med Spine Nerves 2018;13(2):1−10.Article
- [31] Zhen Y, Zhao M, Xiaoxiu M, Lingjun K, Juntao Y. Meta-analysis of the efficacy of Tuina in the treatment of shoulder pain. Shanghai Med Pharma J 2021;42(15):36−9. http://open.oriprobe.com/articles/61724938/Meta_analysis_of_the_efficacy_of_Tuina_in_the_trea.htm.
- [32] Hong S, Do K, Yoon K. Effects of Chuna Manual Therapy (CMT) on Rotator Cuff Disorder: A Systematic Review. J Chuna Man Med Spine Nerves 2021;16(1):1−11.Article
- [33] Cho J, Heo I, Park S, Shin B. Chuna Manual Therapy for Adhesive Capsulitis: A Systematic Review and Meta Analysis. J Chuna Man Med Spine Nerves 2019;14(2):1−14.Article
- [34] Han D, Lee J, Nam S, Son J, Jung D, Jo H. Chuna Manual Therapy for Lateral Epicondylitis: A Systematic Review. J Korean Med Rehabil 2022;32(3):65−75.Article
- [35] Park S-Y, Lee S-H, Heo I, Hwang E-H. Chuna Manual Therapy for Carpal Tunnel Syndrome: A Systematic Review. J Chuna Man Med Spine Nerves −2021. 16(2):9−19.Article
- [36] Lee E-B, Kim H-J, Kim C-Y, Ahn H-D. Effects of Chuna manual therapy after hip arthroplasty: a systematic review and meta-analysis of randomized controlled trials. J Korean Med Rehabil 2022;32(2):95−103.Article
- [37] Xu Z, Gaxi Y, Yuqian P, Xiaxuan C. Meta Analysis of Randomized Controlled Trial of Massage Therapy for Knee Osteoarthritis. J Pract Tradit Chin Intern Med 2023;37(2):157−8. https://caod.oriprobe.com/articles/64173085/tui_na_zhi_liao_xi_guan_jie_gu_xing_guan_jie_yan_a.htm.
- [38] Shengqiang P, Ning L, Junpeng L, Xianf H. The safety and efficacy of massage therapy on knee osteoarthritis: A meta-analysis. J Modern Med Health 2022;38(21):3676−9.
- [39] Liu J, Liu R. Meta Analysis of Knee Osteoarthritis Treatment with Traditional Chinese Massage Combined with Sodium Hyaluronate. J Jiangxi Univ Tradit Chin Med 2021;33(4):27−31.
- [40] Hui X, Lianbo X, Bingxin K. Clinical effecacy and safety of Chinese Tuina in treating knee osteoarthritis Meta-analysis. Shaanxi J Tradit Chin Med 2019;40(12):1807−13.
- [41] Huan Z, Min-jian Y, Wei S, Shu-chao C, Yi-min D. Therapeutic effect of massage on knee osteoarthritis: a meta-analysis. Hainan Med J 2019;30(7):925−9. https://caod.oriprobe.com/articles/56526155/Therapeutic_effect_of_massage_on_knee_osteoarthrit.htm.
- [42] Yang B, Limin X, Quanmao D, Yingpeng X, Dezhi W, Lisu W. Meta-analysis of the efficacy of tuina combined with external Chinese medicine treatment in knee osteoarthritis. Chin J Clin 2018;46(10):1245−7.
- [43] Lee E, Lee Y, Kim H, Ahn H, Yang D. Chuna Manual Therapy for Patients after Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. J Chuna Man Med Spine Nerves 2021;16(1):13−23.Article
- [44] Kwak MK, Kim MW, Jeong SJ, Kim SA, Jeong MY, Kim JH. Systematic Review of Chuna Manipulative Treatment for Ankle Sprain. J Acupunct Res 2018;35(2):61−8.ArticlePDF
- [45] Moon TW, Choi TY, Park TY, Lee MS. Chuna therapy for musculoskeletal pain: A systematic review of randomized clinical trials in Korean literature. Chin J Integr Med 2013;19(3):228−32.ArticlePubMedPDF
- [46] Lee NW, Kim GH, Heo I, Kim KW, Ha IH, Lee JH, et al. Chuna (or Tuina) Manual Therapy for Musculoskeletal Disorders: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Evid Based Complement Alternat Med 2017;2017:8218139. ArticlePubMedPMCPDF
- [47] Lee NW, Lee SH, Kim KW, Ha IH, Cho JH, Lee YJ. Effectiveness of Chuna (or Tuina) Manual Therapy for Temporomandibular Disorder: A Systematic Review. Altern Ther Health Med 2023;29(1):258−68.
- [48] Bae D-R, Cho H-J, Kim H-N, Hwang E-H. Chuna manual therapy for temporomandibular joint disorder: systematic review. J Korean Med Rehabil 2017;27(3):71−9.Article
- [49] He L, Huang H, Wu C, Ding M, Yu M, Qui Z. Meta-analysis of Efficacy and Safety of Meridian Massage in the Treatment of Temporo-mandibular Disorders. J Med Info 2023;36(11):60−6. [in Chinese] http://open.oriprobe.com/articles/65479025/Meta_analysis_of_Clinical_Efficacy_and_Safety_of_M.htm.
- [50] Kim H, Gwon T, Kim B. Chinese Medicine including Chuna Manual Therapy for Osteoarthritis: A Systematic Review. J Chuna Man Med Spine Nerves 2018;13(1):11−21.Article
- [51] Heo I, Han I, Cha Y. Chuna Manual Therapy for Rheumatoid Arthritis : A Systematic Review and Meta-analysis. J Chuna Man Med Spine Nerves 2018;13(1):1−10. http://www.chuna.kr/journal/view.html?uid=293&&vmd=Full.
- [52] Wang Z, Xu H, Zhou H, Lei Y, Yang L, Guo J, et al. A systematic review with meta-analysis: Traditional Chinese tuina therapy for insomnia. Front Neurosci 2023;16:1096003. ArticlePubMedPMC
- [53] Luo SW, Huang NP, Xiang Q, Huang XQ, Tan ZW, Teng X, et al. A systematic review and meta-analysis of acupuncture combined with Tuina in the treatment of insomnia. Medicine (Baltimore) 2022;101(51):e30703. ArticlePubMedPMC
- [54] Dai N, He Q, Liu X, Fang M, Xiong M, Li X, et al. Therapeutic massage/Tuina for treatment of functional dyspepsia: a systematic review and meta-analysis of randomized controlled trials. Qual Life Res 2023;32(3):653−67.ArticlePubMedPDF
- [55] Fang YP, Huang YT, Chen D, Kan Y, Wang JW, Kang XL, et al. Systematic review and Meta analysis on the effectiveness and safety of tuina in treatment of functional constipation [Chinese]. Zhongguo Zhen Jiu 2021;41(6):691−8. [in Chinese].PubMed
- [56] Kim B, Hwang E, Heo I, Lim K, Cho J, Shin B. Chuna Manual Therapy for Adult Constipation : A Systematic Review. J Chuna Man Med Spine Nerves 2016;11(2):23−33. https://scienceon.kisti.re.kr/commons/util/originalView.do?cn=JAKO201624853876652&oCn=JAKO201624853876652&dbt=JAKO&journal=NJOU00295202.
- [57] Fan Z, Di A, Huang F, Zhao S, Qiu M, Wu C, et al. The effectiveness and safety of Tuina for tension-type headache: A systematic review and meta-analysis. Complement Ther Clin Pract 2021;43:101293. ArticlePubMed
- [58] Kim J, Kim B, Kim H, Yook T, Kim J. A Review of Chuna Manual Therapy for Tension Type Headache: Focusing on Pubmed and Korean Literature. J Chuna Man Med Spine Nerves 2016;11(1):1−10. https://koreascience.kr/article/JAKO201620855543300.page.
- [59] Lee D-W, Kim J-Y, Hong M-H, Koo B-S, Kim G-W. A Systematic Review and Meta-Analysis of Randomized Controlled Trials on Chuna Manual Therapy for Cervicogenic Headache. J Orient Neuropsychiatry 2019;30(2):89−105. [in Korean] https://koreascience.kr/article/JAKO201919163088660.page.
- [60] Bu FL, Han M, Lu CL, Liu XH, Wang WG, Lai JL, et al. A systematic review of Tuina for irritable bowel syndrome: Recommendations for future trials. Complement Ther Med 2020;52:102504. ArticlePubMed
- [61] Seo H, Lee H, Hwang M. Chuna Manual Therapy for Irritable Bowel Syndrome; A Systematic Review. J Chuna Man Med Spine Nerves 2016;11(2):1−9. https://www.kci.go.kr/kciportal/ci/sereArticleSearch/ciSereArtiView.kci?sereArticleSearchBean.artiId=ART002186407.
- [62] Song J, Kim J, Nam D. Benefit of chuna for managing symptoms in chronic fatigue syndrome patients: A systematic review and meta-analysis. J Korean Med 2020;41(3):205−20.Article
- [63] Lim K, Hwang E, Kim B, Park I, Heo I. Chuna Manual Therapy for Essential Hypertension : A Systematic Review. J Chuna Man Med Spine Nerves 2017;12(1):29−42. https://www.kci.go.kr/kciportal/ci/sereArticleSearch/ciSereArtiView.kci?sereArticleSearchBean.artiId=ART002239421.
- [64] Yang X, Zhao H, Wang J. Chinese massage (Tuina) for the treatment of essential hypertension: A systematic review and meta-analysis. Complement Ther Med 2014;22(3):541−8.ArticlePubMed
- [65] Seo H, Li Y, Lee J, Kim M. Chuna Manual Therapy for Primary Dysmenorrhea: A Systematic Review. Chuna Manual Therapy for Primary Dysmenorrhea: A Systematic Review. J Korean Rehabil Med 2017;27(3):81−93. [in Korean] http://www.e-jkmr.org/journal/view.html?doi=10.18325/jkmr.2017.27.3.81.Article
- [66] Park S-H, Ko Y-S, Lee J-H. A Study for Indication and Adopted Techniques of Chuna Treatment-Focusing on Domestic Clinical Studies. J Korea Chuna Man Med Spine Nerves 2013;8(2):57−66. [in Korean] https://koreascience.kr/article/JAKO201303536816486.page.
- [67] Park J-M, Shin S-W, Park J-H. A comparative study on the concepts of the Chuna. J Korean Med Classics 2008;21(2):173−91. [in Korean] http://journal.kci.go.kr/jkmc/archive/articleView?artiId=ART001248709.Article
References
Figure & Data
References
Citations
- Reporting Overviews of Reviews: PRIORitizing a Reporting Guideline
Lisa Hartling, David Moher
Perspectives on Integrative Medicine.2024; 3(2): 65. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite