Articles
- Page Path
- HOME > Perspect Integr Med > Volume 2(3); 2023 > Article
-
Protocol
Acupuncture for Rectal Cancer Patients with Low Anterior Resection Syndrome: A Mixed Method Pilot Study Protocol -
Ming Yang1,2,†
 , Honglin Jiang1,2,†, Lin Xu1,2, Qiaoli Zhang1,2, Xun Li3, Liu Han1, Yudong Bao1,2, Lu Yang1,2, Mi Zhang1,2, Lihua Zheng4, Ningyuan Liu4, Jianping Liu3,*, Jinchang Huang1,2,*
, Honglin Jiang1,2,†, Lin Xu1,2, Qiaoli Zhang1,2, Xun Li3, Liu Han1, Yudong Bao1,2, Lu Yang1,2, Mi Zhang1,2, Lihua Zheng4, Ningyuan Liu4, Jianping Liu3,*, Jinchang Huang1,2,* -
Perspectives on Integrative Medicine 2023;2(3):195-201.
DOI: https://doi.org/10.56986/pim.2023.10.008
Published online: October 23, 2023
1Beijing University of Chinese Medicine Third Affiliated Hospital, Beijing, China
2Institute of Acupuncture and Moxibustion in Cancer Care, Beijing University of Chinese Medicine, Beijing, China
3Centre of Evidence-Based Chinese Medicine, Beijing University of Chinese Medicine, Beijing, China
4China-Japan Friendship Hospital, Beijing, China
- *Corresponding authors: Jianping Liu, Centre of Evidence-Based Chinese Medicine, Beijing University of Chinese Medicine, 11 Beisanhuan Dong Lu, Chaoyang District, Beijing, 100029 China, Email: jianping_l@hotmail.com. Jinchang Huang, Beijing University of Chinese Medicine Third Affiliated Hospital, 51 An Wai Xiao Guan Jie, Chaoyang District, Beijing, 100029 China, Email: zryhhuang@163.com
- † The authors contributed equally to this article.
©2023 Jaseng Medical Foundation
This is an open access article under the CC BY-NC license (http://creativecommons.org/licenses/by-nc/4.0/).
- 548 Views
- 12 Download
Abstract
-
Background
- This protocol aims to facilitate the evaluation of acupuncture in the treatment of low anterior resection syndrome (LARS) on the bowel in rectal cancer patients.
-
Methods
- This pragmatic pilot study was designed using a convergent parallel mixed methods design combining a single-arm trial and semi-structured qualitative interview.
-
Results
- Sixty patients with LARS will be recruited from out/inpatient departments. For evaluation of efficacy, the single-arm objective performance criteria will be used in the pilot study in which all eligible participants will receive electroacupuncture mainly on Baliao acupoints three times a week for four weeks. The LARS scale, Memorial Sloan Kettering Cancer Centre Bowel Function Index, and anorectal manometry will be used to assess symptoms and pressure changes. The European Quality of Life Five Dimensions Questionnaire and the European Organization for Research and Treatment of Cancer-Quality of Life Questionnaire-Core 30 will be used to evaluate quality of life. Semi-structured interviews will be conducted among twenty participants to understand their experience and feelings. The qualitative and quantitative data will be analyzed and summarized before comparative analysis. Qualitative themes derived from qualitative analysis will be ranked with the variables of quantitative statistics. Finally, we will answer the research question from multiple perspectives by comparing different types of evidence for the same dimension.
-
Conclusion
- This mixed method study design will potentially evaluate the feasibility and effects of electroacupuncture for LARS and gain an in-depth understanding of the attitudes, experiences, feelings, and acceptance among patients with LARS.
- Low anterior resection syndrome (LARS) is a common postoperative symptom of low rectal cancer patients, which has a high morbidity and severely affects quality of life [1]. In March 2020, the LARS International Collaborative Group released the International Consensus Definition of LARS including eight symptoms and eight consequences [2]. LARS has been reported to affect up to 60%–90% of patients who undergo low or ultralow anterior resection, and can last for several years after surgical treatment [3–5]. Therefore, the quality of life of rectal cancer patients is closely associated with the severity of LARS, and it is necessary to identify effective treatment to improve bowel dysfunction [6].
- According to the management guideline for LARS (MANUEL project in 2021), there are various approaches for the treatment of LARS, including pelvic floor rehabilitation, sacral nerve stimulation, transanal irrigation, and medications. However, all of these approaches have limitations [7,8] (Table 1 [9–14]). At present (July, 2023), there are only 7 relevant studies on LARS identified in the Chinese Clinical Trial Registry (http://www.chictr.org.cn). Therefore, it is of great significance to determine a treatment for LARS with less trauma, low cost, stable effects, and good acceptance. Traditional Chinese medicine (TCM) therapies, especially acupuncture, have been applied to treat LARS in clinical practice, and can directly act on the local lesions and have a positive effect [15–17]. The MANUEL project published in 2021, identified the LARS scale and the Memorial Sloan Kettering Cancer Centre Bowel Function Index in the management guidelines to evaluate LARS [18]. In addition to the quantitative data, LARS also impacts on the mental and emotional wellbeing, and affects social and daily activities [2]. Therefore, mixed methods research should be introduced in order to understand the expectation, experience, acceptability, and superiority of therapy features, to analyze and explain research questions more completely, and to obtain an evaluation consistent with patient experience [19].
- Baliao acupoints are located on the foot bladder meridian and the branch meridian goes into anus. Acupuncture at Baliao points can assist pelvic floor muscle contraction, stimulate sacral nerve and pubic nerve and promote the recovery of anorectal function, and the cost and trauma are much less than sacral nerve stimulation therapy. Electroacupuncture can provide constant electrical stimulation and it is an effective treatment in clinical practice.
- This protocol set out a study which aims to explore the effect of acupuncture for rectal cancer patients with LARS initially by applying a mixed method research design to provide a broader deeper knowledge, and evidence for future trials and clinical practice.
Introduction
- 1. Study design and setting
- This pragmatic study is a convergent parallel mixed methods design [20], including quantitative research and qualitative research, which will be carried out independently and in parallel. After analyzing quantitative and qualitative data we plan to synthesize and further analyze the results through comparison or transformation. The quantitative research uses objective performance criteria [21], and the qualitative research uses semi-structured qualitative interviews.
- In the single-arm trial, participants who meet the inclusion and exclusion criteria will be recruited from the Department of Acupuncture and Minimally Invasive Oncology (out/inpatients) in Beijing University of Chinese Medicine Third Affiliated Hospital. Before the research starts, investigators will introduce this research program to the patients, acquire their informed written consent, and record their baseline data.
- In the qualitative research, purposive (selective) sampling [22] will be adopted to conduct semi-structured qualitative interviews within the scope of participants in the single-arm trial who have good communication and understanding, able to report outcomes independently, and able to be investigated by qualitative interview.
- From April 2023, a total of 60 eligible patients will be recruited. Every potential participant will be invited to take part in the study and make an informed decision after assessing the benefits and burdens of the study.
- 2. Participants
- This study will be conducted on patients aged 18–75 years who have LARS. Detailed inclusion criteria and exclusion criteria are shown as follows:
Aged 18–75, no gender limitation.
Meet the LARS diagnostic criteria, LARS score ≥ 20.
KPS score ≥ 60, expected survival > 3 months, no staging and metastasis limitation.
Agreed to participate in the study and signed the informed consent.
With past medical history: other anorectal surgery or trauma, spinal cord, brain, and other nerve injuries which make patients unable to control defecation, serious complications, and anaphylactic reactions or adverse events occurred during acupuncture which make patients unable to tolerate acupuncture.
With complications: other anorectal diseases, anastomotic leakage, anastomotic bleeding, anastomotic stenosis, and intestinal perforation.
Receiving other acupuncture treatment.
With sacral malformation by any reason leading to inaccurate acupuncture point positioning.
Presence of other diseases: serious primary diseases of the cardiovascular, liver, kidney and hematopoietic systems and mental disorders.
Participating in other clinical studies.
With serious adverse events during treatment.
With aggravation and emergencies during treatment.
Failed to complete the treatment course and observation period specified in the study protocol for some reason.
Refuse to continue participating in the study or drop out of the study.
- 3. Interventions
- The acupuncture operation in this single-arm study follows the theory of meridians and collaterals in TCM. In clinical practice, electroacupuncture was determined to be beneficial for LARS control, and the researches on acupuncture for defecation dysfunction after sphincter-preserving surgery for rectal cancer also showed potential effects [23].
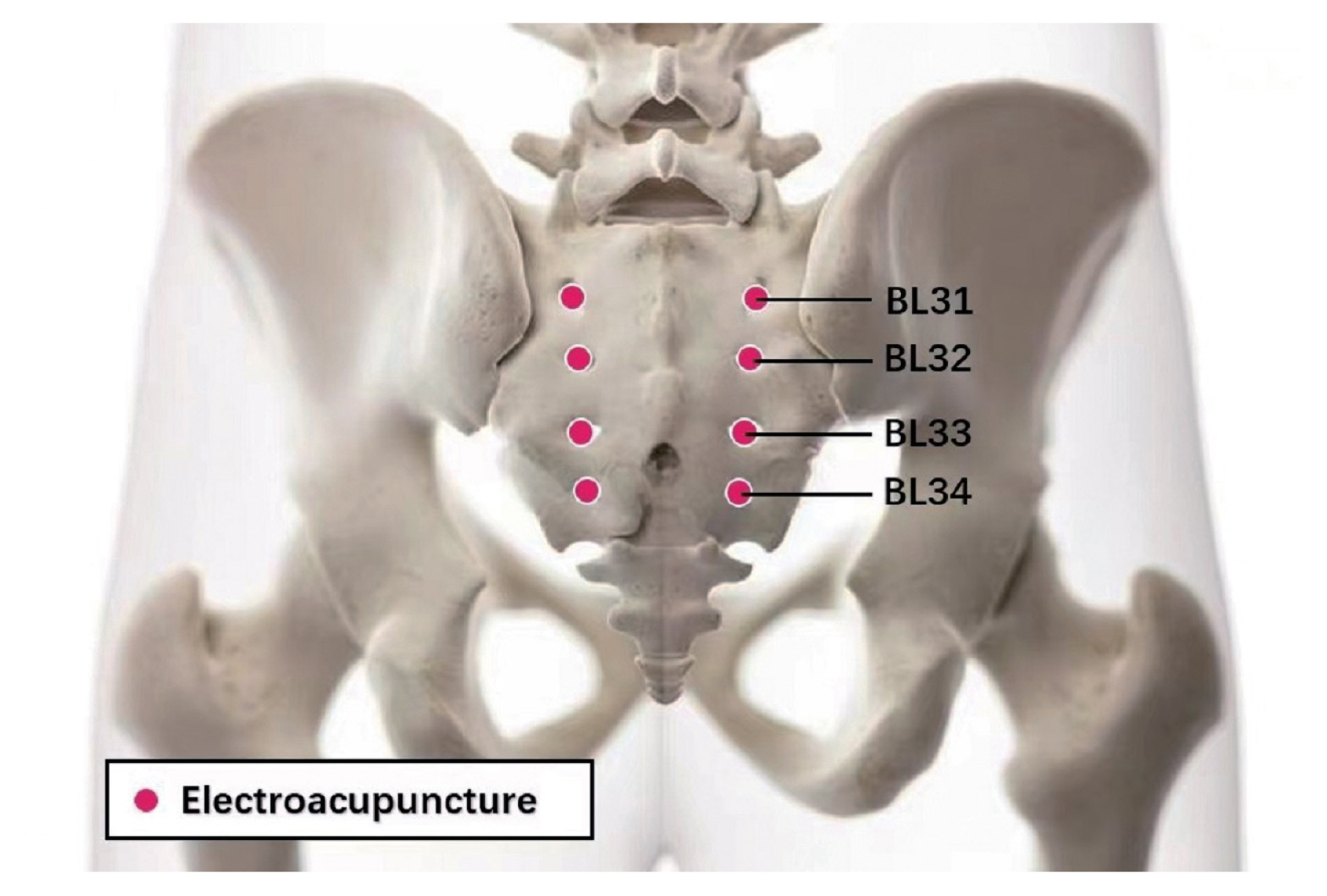
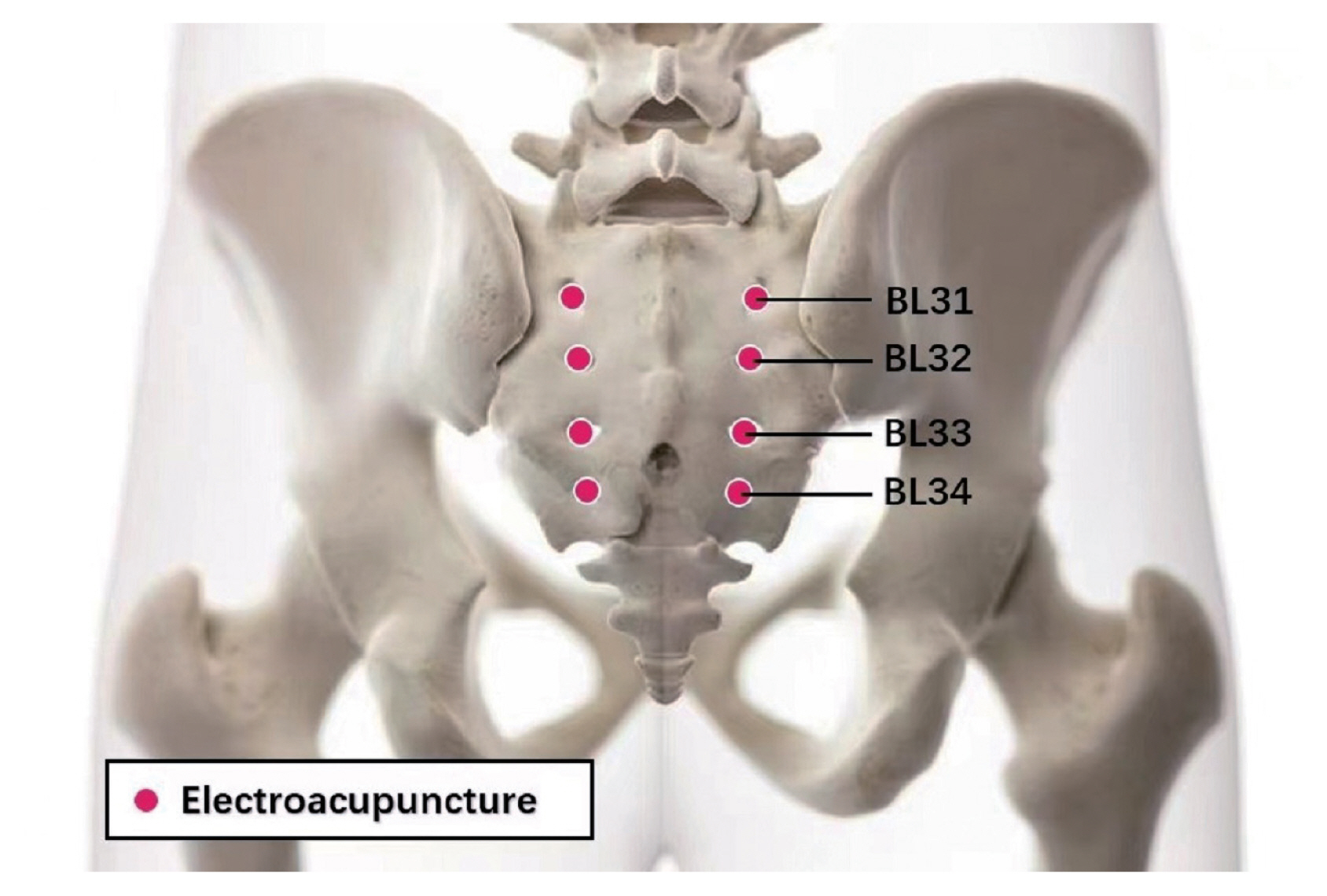
- Disposable acupuncture needles 0.30 × 75 mm (Hwato) and SDZ-V electroacupuncture apparatuses (Hwato) will be used. Participants will receive acupuncture at Baliao (BL31, BL32, BL33, BL34, bilateral, total of 8 acupoints; Fig. 1) [24,25] . Baliao is located in the 1st to 4th sacral foramen. Acupuncture at Baliao can directly stimulate the sacral nerve, exert a positive and extensive neuro-humoral regulation effect on the pelvic floor anorectal organs through complex nerve connections, and contribute to the recovery of defecation function [26]. After skin disinfection, following needle insertion, small, equal manipulations of twirling, lifting, and thrusting will be performed on all needles to reach Deqi (a composite of sensations including soreness, numbness, distention, heaviness, and other sensations), which is believed to be an essential component for acupuncture. The acupuncture depth of Shangliao (BL31), Ciliao (BL32), Zhongliao (BL33) and Xialiao (BL34) is about 50 mm (2 cun), 50 mm (2 cun), 40 mm (1.5 cun) and 40 mm (1.5 cun), respectively. The electroacupuncture stimulation will last for 30 minutes with a continuous wave of 50 Hz and a current intensity of 1–5 mA (preferably with the skin around the acupoints mildly quivering without pain). Participants will receive 3 treatment sessions per week for 4 consecutive weeks, 12 sessions in total.
- In addition to acupuncture at Baliao points, acupoints can be selected according to the patient’s syndrome differentiation. No more than 3 acupoints will be selected according to syndrome differentiation.
- The physicians will be trained for this project and have a certificate to show they are qualified as a practicing physician of TCM, professional knowledge of oncology of integrative traditional Chinese and Western medicine, at least 2 years of clinical experience in acupuncture treatment of tumors, and training experience in acupuncture.
- Except for the intervention with acupuncture, patients will be recommended to avoid other Chinese/Western medicines or treatment methods related to the disease during the study period. If necessary, antidiarrheal drugs (anti-gastrointestinal motility drug lepidine capsules) can be used as a rescue measure for severe LARS patients. Drugs that must be continued due to other diseases may remain unchanged.
- Regardless of whether the combined intervention taken by patients is related to LARS treatment, the drug name/therapies, dosage, frequency, and duration of treatment shall be recorded for analysis and reporting in summary.
- 4. Outcome
- Using the LARS scale [27], the severity of urgency, frequency, clustering, incontinence for flatus, and incontinence for liquid stool will be scored, 0–20 is classified as no LARS, 21–29 as mild, and 30–42 as severe LARS.
- Secondary outcomes will be measured using the Memorial Sloan Kettering Cancer Centre Bowel Function Index scale [28], Anorectal pressure test [29], European Quality of Life Five Dimensions Questionnaire [30], and the European Organization for Research and Treatment of Cancer-Quality of Life Questionnaire-Core 30 scale [31]. Following at least 2 weeks of treatment, patients who are willing to cooperate with the interview will be selected for semi-structured qualitative interview. The ideal number of interviewees is 20. The interview outline will be as follows:
What was the main discomfort that you thought would bother you before receiving acupuncture treatment? What other approaches have you tried?
Why did you choose acupuncture?
What problems associated with LARS were most alleviated following treatment? After how many treatments was acupuncture beneficial? What was the biggest change in your life as a result of the treatment?
Did you have any discomfort from acupuncture treatment? Do you have any safety concerns?
Would you recommend acupuncture to other LARS patients? How would you introduce the treatment? Under what circumstances would you recommend acupuncture for LARS?
Do you have any suggestions or opinions on acupuncture as an intervention for LARS? What are the disadvantages of acupuncture treatment? What needs to be improved?
- The treatment period will be 4 weeks, and the follow-up points will be 1, 3 and 6 months after the end of the 4-week treatment period. However, the actual follow-up time could be within a week before or after the follow-up point. Outcomes in the follow-up period will include assessment of the LARS score and European Quality of Life Five Dimensions Questionnaire scale at each time point performed over the telephone.
- 5. Timeline of participants
- The timeline for the single-arm trial is depicted in Table 2.
- 6. Sample size estimation
- Single-arm trial: Single-arm objective performance criteria will be used in the quantitative part of the study. The target value will be a LARS score improvement in 60% of the participants. This value was reached because if the effective rate of the intervention reaches 60% or above, it can be preliminarily considered that this therapy has a potential valuable effect. Based on previous clinical practice, the overall incidence of LARS score improvement in acupuncture intervention in patients is expected to be 80%. According to the approximate normal method and considering a shedding rate of 10%, the sample size should be 60 participants [21]. Qualitative research: The minimum empirical sample size should not be less than 20, so 20 interviewees will be selected.
- 7. Recruitment
- Participants will be recruited by using advertisements through press release, posting recruitment advertisements at study institution, and using an online recruitment announcement.
- 8. Data management
- Quantitative research data will be inputted into the REDCap system for data collection and management [32,33]. Qualitative research data will be audio-recorded and transcribed by the authors verbatim. Any private detail concerning individual participants will be anonymized. Thematic analysis [34,35] will be undertaken, and open coding will be carried out independently. The codes will then be categorized, redundant or unnecessary codes will be merged in the process, and the codebook will be updated. Nvivo11 (QSR International) is a qualitative data analysis package which will be used for data storage and management.
- 9. Statistical analysis
- This study is a convergent parallel mixed methods design, which combines quantitative and qualitative data to compare results. The specific steps are as follows [20]:
Conduct quantitative and qualitative analysis independently.
According to the latest LARS diagnostic criteria, LARS patients have at least one of the 8 symptoms and one of the 8 consequences [2]. “Symptoms” and “Consequences” can be considered as two dimensions of convergent parallel design, and the eight symptoms and eight outcomes can be compared in these two dimensions. If new dimensions and information are discovered in the qualitative interview, it can be added appropriately.
Generate information to be compared and present these comparisons.
- 10. Adverse events
- All adverse events (AEs) that occur during the study will be checked and recorded. AEs are any undesirable and unintentional signs (e.g., broken needle, fainting, skin infections, hemorrhage, hematoma, other systemic discomfort after acupuncture), symptoms, or illnesses that occur after the procedures in the course of the study, which do not necessarily have a causal relationship with the treatment. AEs will be collected through participants’ complaints or by monitoring the participants. AEs between groups will be reported by frequency.
- 11. Ethical consideration and dissemination
- After screening, we will invite potentially eligible patients to participate in the study. Before the research starts, informed consent will be obtained from all participants and/or their legal guardian(s). All the involved procedures, probable benefits, and potential risks will be elaborated. They will also be informed that participation in the study is entirely voluntary and their treatment will not be influenced if they refuse to take part. All questions and worries raised will be explained in detail. Only after informed written consent obtained, patients who meet the inclusion criteria but not the exclusion criteria, can be recruited. The personal information of all the participants will always be kept confidential. Serial numbers rather than their real names will be used when data is analyzed.
Materials and Methods
2.1. Inclusion criteria
2.2. Exclusion criteria
2.3. Dropout criteria
3.1. Acupuncture intervention
3.2. Co-intervention
4.1. Primary outcomes
4.2. Secondary outcomes
11.1. Patient consent
- LARS is a common complication after the total mesorecta excision surgery. However, there is little attention on LARS in China, only 7 relevant studies have been found in the Chinese Clinical Trial Registry and no relevant qualitative research has been found. Therefore, it is of great significance for LARS to find a treatment with less trauma, stable effects, and good acceptance. In clinical practice, Baliao acupoints have been reported as effective for LARS and the effect on pelvic floor-related conditions/disease was reported in a previous RCT [36]. In this exploratory mix-method study, single-arm trial will be adopted to assess the intervention effect, and the qualitative part could investigate an in-depth understanding of the feasibility of acupuncture treatment of LARS of rectal cancer, the attitudes, experiences, feelings, and acceptance of different patients.
- All the bias will be controlled maximally and the study could offer a new way for patients suffering LARS.
Discussion
Acknowledgments
-
Author Contributions
Conceptualization,funding acquisition, methodology, writing-original draft, writing - review & editing: MY. Conceptualization, methodology, writing-original draft, writing - review & editing: MY. Resources, investigation, methodology, writing - review & editing: LX and QLZ. Conceptualization, methodology, software, writing - review & editing: XL. Methodology, resources, writing - review & editing: LH. Investigation, writing-review & editing: YDB, LY, and MZ. Resources, writing-review & editing: LHZ and NYL. Conceptualization, methodology, resources, supervision, writing-review & editing: JPL and JCH.
-
Conflicts of Interest
The authors have no conflicts of interest to declare.
-
Funding
The Capital’s Funds for Health Improvement and Research (no.: CFH2022-4-7046).
-
Ethical Statement
This protocol has been approved by the Institutional Review Board of the Third School of Clinical Medicine, Beijing University of Chinese Medicine (no.: BZYSY-2022KYKTPJ-07-XZ01). The protocol was registered on ISRCTNregistry (no.: ISRCTN12537763). Registered on 16 August 2022, https://www.isrctn.com/ISRCTN12537763. Any revision will be updated to the mentioned website.
Article information
Data Availability
Trial Status
| Year of publication [refs] | Method | Outcomes | N | No. original studies | Type of research |
|---|---|---|---|---|---|
| 2018 [9–10] | Diet and drugs | No significant effect was observed after taking probiotics, 5-HT3 improves WEXNER score | 25 | 2 | Case series |
| 2014 [11] | Pelvic floor rehabilitation | Results without LARS score, improved Cleveland incontinence score and FACT-C score had different degrees of benefit | 321 | 5 | Systematic reviews of included cohort studies |
| 2020 [12] | Transanal irrigation | No significant difference in LARS scores at 12 months | 37 | 1 | RCT |
| 2018 [13] | Antegrade enema | 88% of patients treated did not need an ostomy in the long term | 25 | 1 | Case series |
| 2015 [14] | Sacral nerve stimulation | Symptom improvement in 74% of patients (ITT analysis) | 43 | 7 | Systematic reviews of included case series |
5-HT3 = 5-hydroxytryptamine receptor antagonist; WEXNER score = fecal incontinence severity score; LARS = low anterior resection syndrome; FACT-C = Quality of Life Scale for Patients with Colorectal cancer; ITT analysis = intentionality analysis (whether the treatment was eventually included in the assigned group for statistical analysis of efficacy); RCT = randomized controlled trials.
LARS = Low anterior resection syndrome; MSKCC BFI = The Memorial Sloan-Kettering Cancer Center Bowel Function Instrument; EQ-5D = European Quality of live Five Dimensions Questionnaire; EORTC-QLQ-C30 = The European Organization for Research and Treatment of Cancer-Quality of Life Questionnaire-Core 30.
Considering the ethical principles and patient compliance = only some participants with mild LARS (around 15 people) will be selected for the anorectal pressure test. Safety and adverse events will be local and systemic adverse events of the intervention. Hematuria and stool routine = liver and kidney function = and infection will be tested at baseline and after the intervention. After at least 2 weeks of treatment = about 20 patients who are willing to cooperate with the interview will be selected for semi-structured qualitative interview.
- [1] Si CS, Yang L. Hot issues of organ reservation in low and middle stage locally advanced rectal cancer. Chin J Surg Oncol 2021;13(2):109−12. [in Chinese].
- [2] Keane C, Fearnhead NS, Bordeianou LG, Christensen P, Basany EE, Laurberg S, et al, LARS International Collaborative Group. International Consensus Definition of Low Anterior Resection Syndrome. Dis Colon Rectum 2020;63(3):274−84.ArticlePubMedPMC
- [3] Chen TY, Emmertsen KJ, Laurberg S. Bowel dysfunction after rectal cancer treatment: a study comparing the specialist’ s versus patient’s perspective. BMJ Open 2014;4(1):e003374. ArticlePubMedPMC
- [4] Battersby NJ, Juul T, Christensen P, Janjua AZ, Branagan G, Emmertsen KJ, et al, United Kingdom Low Anterior Resection Syndrome Study Group. Predicting the Risk of Bowel-Related Quality-of-Life Impairment After Restorative Resection for Rectal Cancer: A Multicenter Cross Sectional Study. Dis Colon Rectum 2016;59(4):270−80.PubMed
- [5] Qin Q, Huang B, Cao W, Zhou J, Ma T, Zhou Z, et al. Bowel Dysfunction After Low Anterior Resection with Neoadjuvant Chemoradiotherapy or Chemotherapy Alone for Rectal Cancer: A Cross-Sectional Study from China. Dis Colon Rectum 2017;60(7):697−705.ArticlePubMed
- [6] Juul T, Ahlberg M, Biondo S, Espin E, Jimenez LM, Matzel KE, et al. Low anterior resection syndrome and quality of life: an international multicenter study. Dis Colon Rectum 2014;57(5):585−91.PubMed
- [7] Christensen P, Im Baeten C, Espín-Basany E, Martellucci J, Nugent KP, Zerbib F, et al. Management guidelines for low anterior resection syndrome - the MANUEL project. Colorectal Dis 2021;23(2):461−75.ArticlePubMedPMCPDF
- [8] Yu KX, Luo C, Wang XD, Li L. Anal function rehabilitation after rectal cancer surgery. Chin J Colorectal Dis 2021;10(3):298−301. [in Chinese] https://zhjzcjbdzzz.cma-cmc.com.cn/EN/10.3877/cma.j.issn.2095-3224.2021.03.013.
- [9] Stephens JH, Hewett PJ. Clinical trial assessing VSL#3 for the treatment of anterior resection syndrome. ANZ J Surg 2012;82(6):420−7.ArticlePubMed
- [10] Itagaki R, Koda K, Yamazaki M, Shuto K, Kosugi C, Hirano A, et al. Serotonin (5-HT3) receptor antagonists for the reduction of symptoms of low anterior resection syndrome. Clin Exp Gastroenterol 2014;7:47−52.PubMedPMC
- [11] Visser WS, Te Riele WW, Boerma D, van Ramshorst B, van Westreenen HL. Pelvic floor rehabilitation to improve functional outcome after a low anterior resection: a systematic review. Ann Coloproctol 2014;30(3):109−14.ArticlePubMedPMC
- [12] Rosen HR, Boedecker C, Fürst A, Krämer G, Hebenstreit J, Kneist W. “Prophylactic” transanal irrigation (TAI) to prevent symptoms of low anterior resection syndrome (LARS) after rectal resection: results at 12-month follow-up of a controlled randomized multicenter trial. Tech Coloproctol 2020;24(12):1247−53.ArticlePubMedPDF
- [13] Didailler R, Denost Q, Loughlin P, Chabrun E, Ricard J, Picard F, et al. Antegrade Enema After Total Mesorectal Excision for Rectal Cancer: The Last Chance to Avoid Definitive Colostomy for Refractory Low Anterior Resection Syndrome and Fecal Incontinence. Dis Colon Rectum 2018;61(6):667−72.ArticlePubMed
- [14] Ramage L, Qiu S, Kontovounisios C, Tekkis P, Rasheed S, Tan E. A systematic review of sacral nerve stimulation for low anterior resection syndrome. Colorectal Dis 2015;17(9):762−71.ArticlePubMed
- [15] Tian Y, Guan ZA. Research progress of TCM treatment for rectal cancer patients with LARS. Chin J Surg Integr Tradit Western Med 2021;27(2):342−5. [in Chinese].
- [16] Li KX. [Dissertation]. Systematic evaluation and clinical observation of TCM treatment for rectal cancer patients with LARS Beijing (China), Beijing University of Chinese Medicine. 2021;[in Chinese].
- [17] Gui L, Liu YX, Guo LL, Kong B. Acupuncture in the treatment of low and middle anterior resection syndrome. Liaoning J Tradit Chin Med 2010;37(8):1579−80. [in Chinese] https://caod.oriprobe.com/articles/32377658/The_Acupuncture_moxibustion_Treatment_for_Patients_with_Anterior_Resec.htm.
- [18] Christensen P, Im Baeten C, Espín-Basany E, Martellucci J, Nugent KP, Zerbib F, et al. Management guidelines for low anterior resection syndrome - the MANUEL project. Colorectal Dis 2021;23(2):461−75.ArticlePubMedPMCPDF
- [19] Xu JP, Zhang XY, Hu T. Transcending quantitative and qualitative research: Types and applications of mixed methods. J Soochow Univ 2019;7(1):50−9. [in Chinese] https://caod.oriprobe.com/articles/55950609/Beyond_Quantitative_and_Qualitative_Researches_The.htm.
- [20] John W, Cresswell L, Plano C. [Dissertation]. Designing and Conducting: Mixed Methods Research 2nd ed. Chongqing (China), Chongqing University Press. 2017.
- [21] Tang XR, Huang YH, Wang Y, Li W. Comparison of sample size calculation methods for single-arm OPC trials. Chin J Dis Control Prevent 2013;17(11):993−6. [in Chinese] https://caod.oriprobe.com/articles/40421184/Comparison_of_sample_size_calculation_methods_for_single_arm_OPC_trial.htm.
- [22] Liu JP. Qualitative Research Methodology in Evidence-based Chinese Medicine. Beijing (China), People’s Medical Publishing House (PMPH), 2009, p 51.
- [23] Xu G, Xiao Q, Lei H, Fu Y, Kong J, Zheng Q, et al. Effectiveness and safety of acupuncture and moxibustion for defecation dysfunction after sphincter-preserving surgery for rectal cancer: protocol for systematic review and meta-analysis. BMJ Open 2020;10(5):e034152. ArticlePubMedPMC
- [24] Cai HH, Wang LL. Baliao acupoints deep stabbing and its clinical application by professor Wang Lingling. Chin Acupunct Moxibustion 2014;34(3):285−8. [in Chinese].
- [25] Li BW. [Dissertation]. Study on clinical operation standard and local anatomical structure of Baliao acupoints Changchun (China), Changchun University of Traditional Chinese Medicine. 2014;[in Chinese].
- [26] Long ZJ, Guan LC. Application of Baliao Point lengthening Qiang Point in anorectal neurosis. Chin J Integr Tradit Western Med Digest 2014;22(9):547−8. [in Chinese] https://caod.oriprobe.com/articles/42905988/ba_zuo_xue_jia_chang_qiang_xue_zai_gang_men_zhi_chang_shen_jing_guan_n.htm.
- [27] Hou XT, Pang D, Lu Q, Yang P, Jin SL, Zhou YJ, et al. Validation of the Chinese version of the low anterior resection syndrome score for measuring bowel dysfunction after sphincter-preserving surgery among rectal cancer patients. Eur J Oncol Nurs 2015;19(5):495−501.ArticlePubMed
- [28] Hou XT, Pang D, Lu Q, Tian SH, Zhou YJ. Reliability and validity of the MSKCC Bowel Function Instrument in a sample of Chinese rectal cancer patients undergoing sphincter-preserving surgery. Chin J Nurs 2014;49(12):1453−8. [in Chinese] https://caod.oriprobe.com/articles/43710700/Reliability_and_validity_of_the_MSKCC_Bowel_Functi.htm.
- [29] Deng G, Xu LS, Zhang XN, Wu GR. Application of three-dimensional high resolution anorectal manometry and biological feedback therapy in very elderly patients with functional constipation. Chin J Geriatrics 2021;40(5):618−22. [in Chinese].
- [30] Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res 2011;20(10):1727−36.ArticlePubMedPMCPDF
- [31] Wan CH, Chen MQ, Zhang CZ, Tang XL, Meng Q, Zhang XX. Evaluation of the Chinese version of the Cancer Quality of Life Scale EORTC QLQ-C30. J Pract Oncol 2005;(4):353−5. [in Chinese].
- [32] Geng H, Tian GX, He HR, Ma M, Wang Y, Zeng XT. How to safely implement data entry and storage in REDCap system. Chin J Evid Based Cardiovasc Med 2018;10(3):262−4. [in Chinese] https://caod.oriprobe.com/articles/53575895/How_to_achieve_the_data_input_and_storage_of_REDCa.htm.
- [33] Li M, Tian GX, He HR, Geng H, Zeng XT, Lv J. How to use REDCap to input and manage repeated measurement data. Chin J Evid Based Cardiovasc Med 2018;10(6):647−50. [in Chinese] https://caod.oriprobe.com/articles/54971483/How_to_realize_the_repeated_measurement_data_entry.htm.
- [34] Brauni V, Clarke V. Using thematic analysis in Psychology. Qual Res Psychol 2006;3(2):77−101.Article
- [35] Green J, Thorogood N. Qualitative methods for health research. London (UK), Sage, 2004, pp 175−180.
- [36] Liu Z, Liu Y, Xu H, He L, Chen Y, Fu L, et al. Effect of Electroacupuncture on Urinary Leakage Among Women with Stress Urinary Incontinence: A Randomized Clinical Trial. JAMA 2017;317(24):2493−501.ArticlePubMedPMC
References
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite