Articles
- Page Path
- HOME > Perspect Integr Med > Volume 3(1); 2024 > Article
-
Original Article
Acupuncture Needles and the Risk of Lymphedema After Breast Cancer Surgery: A Retrospective National Cohort Study -
Ye-Seul Lee1
 , Yucheol Lim1,2, Jiyoon Yeo3
, Yucheol Lim1,2, Jiyoon Yeo3 -
Perspectives on Integrative Medicine 2024;3(1):29-36.
DOI: https://doi.org/10.56986/pim.2024.02.004
Published online: February 22, 2024
1Jaseng Spine and Joint Research Institute, Jaseng Medical Foundation, Seoul, Republic of Korea
2School of Pharmacy, Sungkyunkwan University, Suwon, Republic of Korea
3Graduate School, Department of Economics, Korea University, Seoul, Republic of Korea
- *Corresponding author: Ye-Seul Lee, Jaseng Spine and Joint Research Institute, Jaseng Medical Foundation, 2F Vision Tower 540 Gangnam-daero, Gangnam-gu, Seoul 06110, Republic of Korea, Email: yeseul.j.lee@gmail.com
©2024 Jaseng Medical Foundation
This is an open access article under the CC BY-NC license (http://creativecommons.org/licenses/by-nc/4.0/).
- 597 Views
- 23 Download
Abstract
-
Background
- Controversies remain over the impact of using needles on breast cancer patients after surgery due to risk of breast cancer-related lymphedema (BCRL). While recent literature suggests that vascular access during the postsurgical stage does not affect the risk of BCRL, the impact of acupuncture on the risk of BCRL during the postsurgical stage has not been studied.
-
Methods
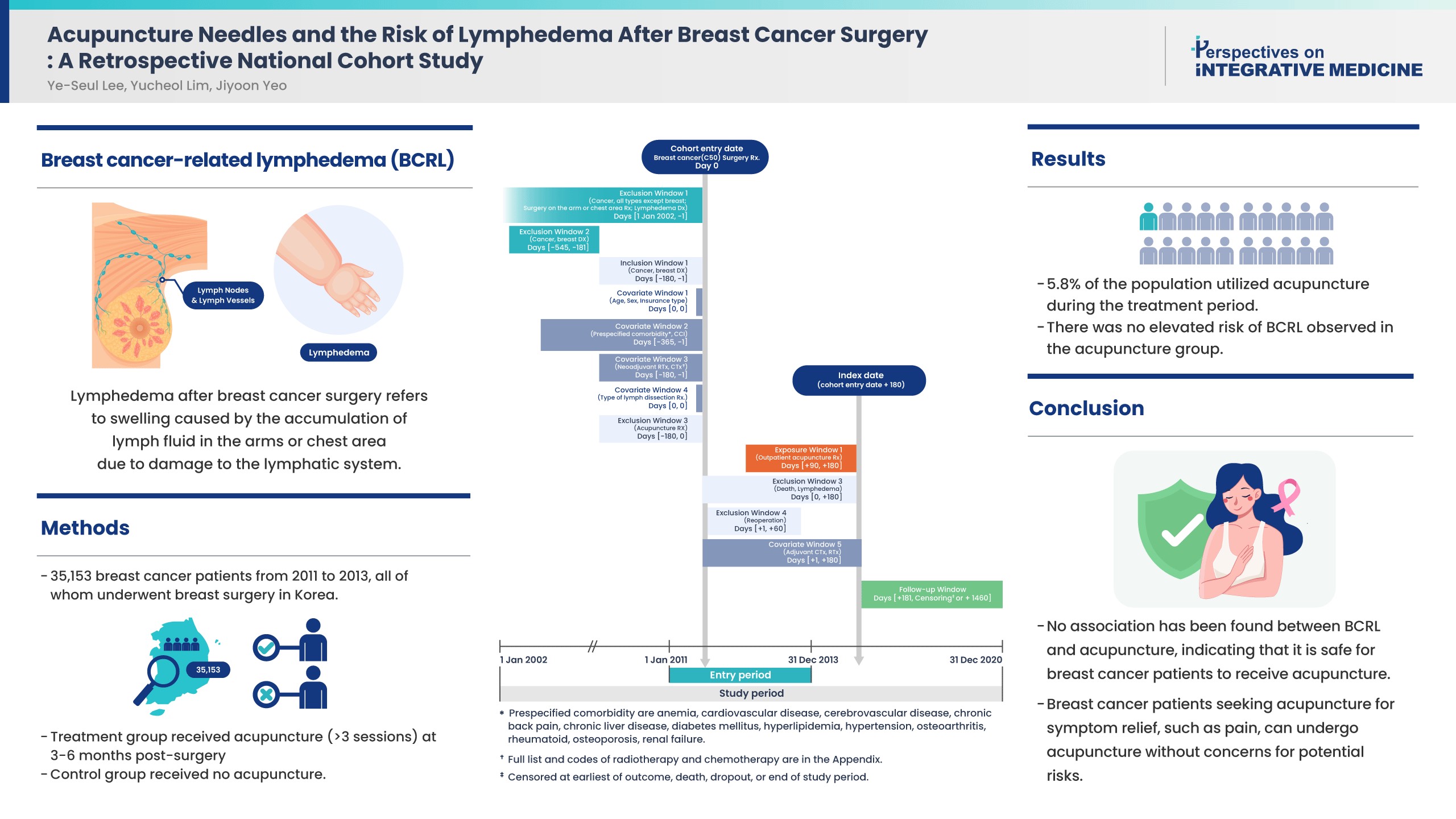
- This study included 35,153 patients from 2011 to 2013 who were newly diagnosed with breast cancer in a population-based cohort from the Korean National Health Insurance Service database. All patients received breast surgery, and the treatment group received acupuncture for more than 3 sessions in the 3–6 months post-surgery. The control group did not receive acupuncture. The incidence rate ratio, Kaplan-Meier curve, and Cox proportional hazards models were used to compare the risk of BCRL, and death between groups.
-
Results
- About 5.8% of the study population received acupuncture during the 3–6 months post-surgery treatment window. After propensity score matching, the acupuncture treatment group did not show an increased risk of BCRL (IRR 1.017, 95% CI 0.868–1.193; unadjusted HR 1.018, 95% CI 0.868–1.193). This risk was robust in all multivariate Cox proportional hazards models.
-
Conclusion
- An association of BCRL with acupuncture was not observed. Patients who received acupuncture to manage symptoms such as pain during the 3–6 months postsurgical stage did not have a higher risk of developing BCRL. Breast cancer patients who seek acupuncture to alleviate post-surgery symptoms such as pain, can receive acupuncture without concerns for potential risk of BCRL.
- The most common complication of breast cancer surgery is upper limb breast cancer-related lymphedema (BCRL), a chronic condition with a substantial impact on the quality of life of breast cancer survivors [1–3]. With a prevalence ranging from 20% to more than 50%, individual characteristics including body mass index, age, and underlying comorbidities influence incidence; furthermore, treatments such as administration of chemotherapy or radiotherapy are factors for BCRL [1–3].
- The avoidance of using needles (for dermal puncture and venipuncture) on the arm affected by breast cancer surgery is commonly practiced among clinicians due to the risk of infection and complications, but the rationale behind this strategy lacks solid evidence and is largely based on anecdotal information. Despite limited evidence supporting its effectiveness [4], institutional policies and clinical guidelines often advocate for this practice simply because there is no proven alternative for reducing the risk of BCRL. Consequently, procedures involving vascular access, such as blood draws and intravenous infusions, have been a topic of debate. However, recent studies, including large cohort studies, have reported no significant association between avoidance of using needles on the arm affected by breast cancer surgery and the development of BCRL [5–7].
- Acupuncture is a non-pharmacological intervention using needles that is increasingly used for the management of various symptoms of breast cancer patients including hot flashes [8–10], nausea [11–13], and pain [14,15]. However, concerns remain over the potential risk of BCRL among breast cancer patients who receive acupuncture during the postsurgical stage. Previous studies investigating the risk of BCRL have mainly examined the influence of intravenous needle insertion. Large cohort studies have yet to be conducted to examine whether there is an association between the use of acupuncture needles and the risk of BCRL.
- This study is a retrospective, nationwide, 10-year cohort study investigated the potential risk of BCRL in patients who received acupuncture as part of their postsurgical adjuvant symptom management therapy. By examining whether there is a risk, the study aimed to cast light on the safety of acupuncture as a complementary treatment for breast cancer survivors seeking further pain management.
Introduction
- 1. Data source
- This was a nationwide, retrospective cohort study utilizing the National Health claims database built by the National Health Insurance Service (NHIS) of Korea. This database contains information from 97.0% of the population who are subscribed to the NHIS [16], a single insurer offering universal healthcare coverage. The remaining 3.0% of the population received Medical Aid [17], and the date of death was accessed from Korean Statistics (government organization responsible for managing national statistics in South Korea). The related materials and metadata are open to the public on the National Health Insurance Data Sharing Service homepage (http://nhiss.nhis.or.kr) [18]. Access to this database is granted upon review by the NHIS inquiry committee for research support. The Institutional Review Board of Gachon University granted a formal waiver for consent (no.: 1044396-202101-HR-001-01).
- 2. Cohort design and study population
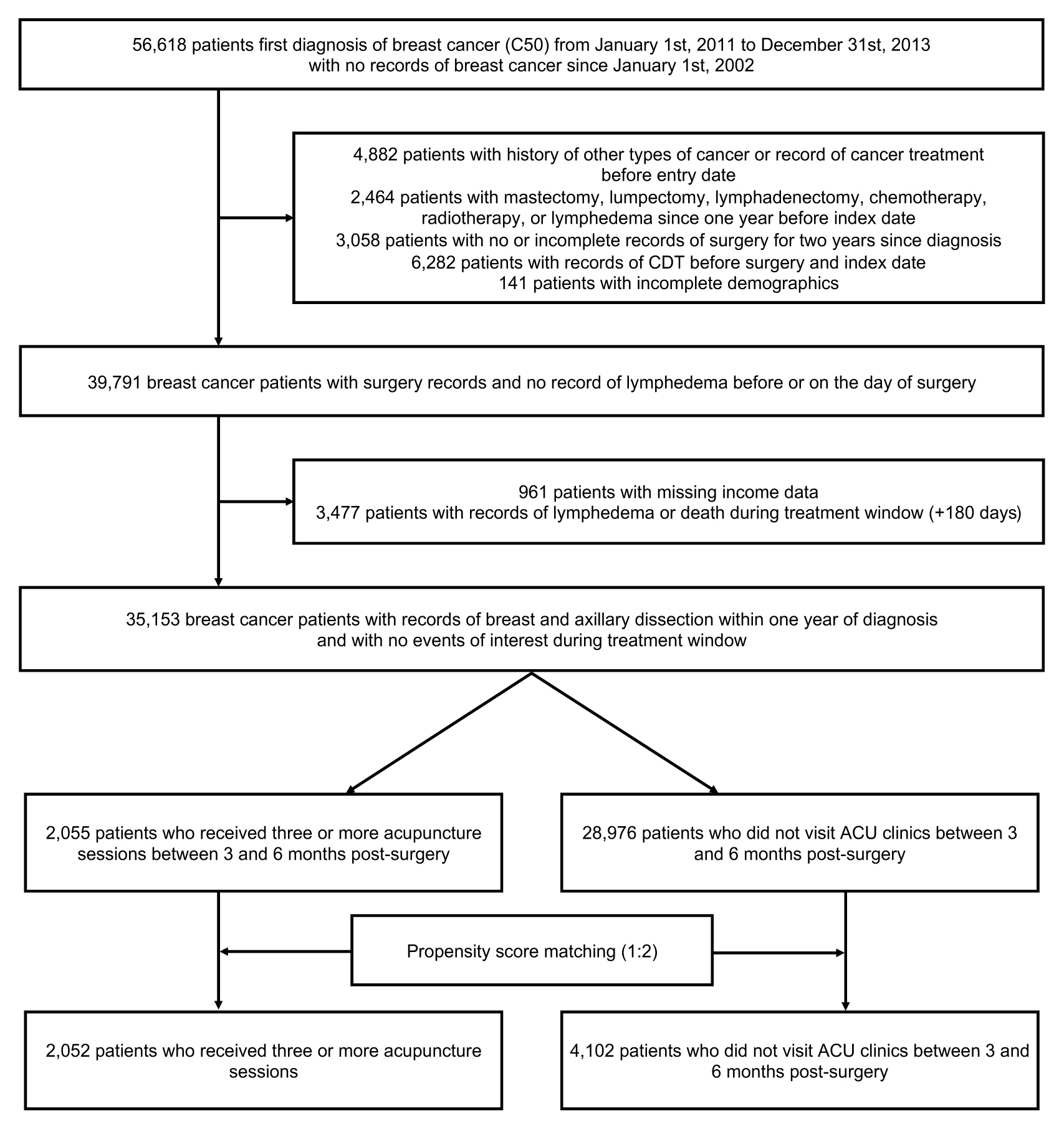
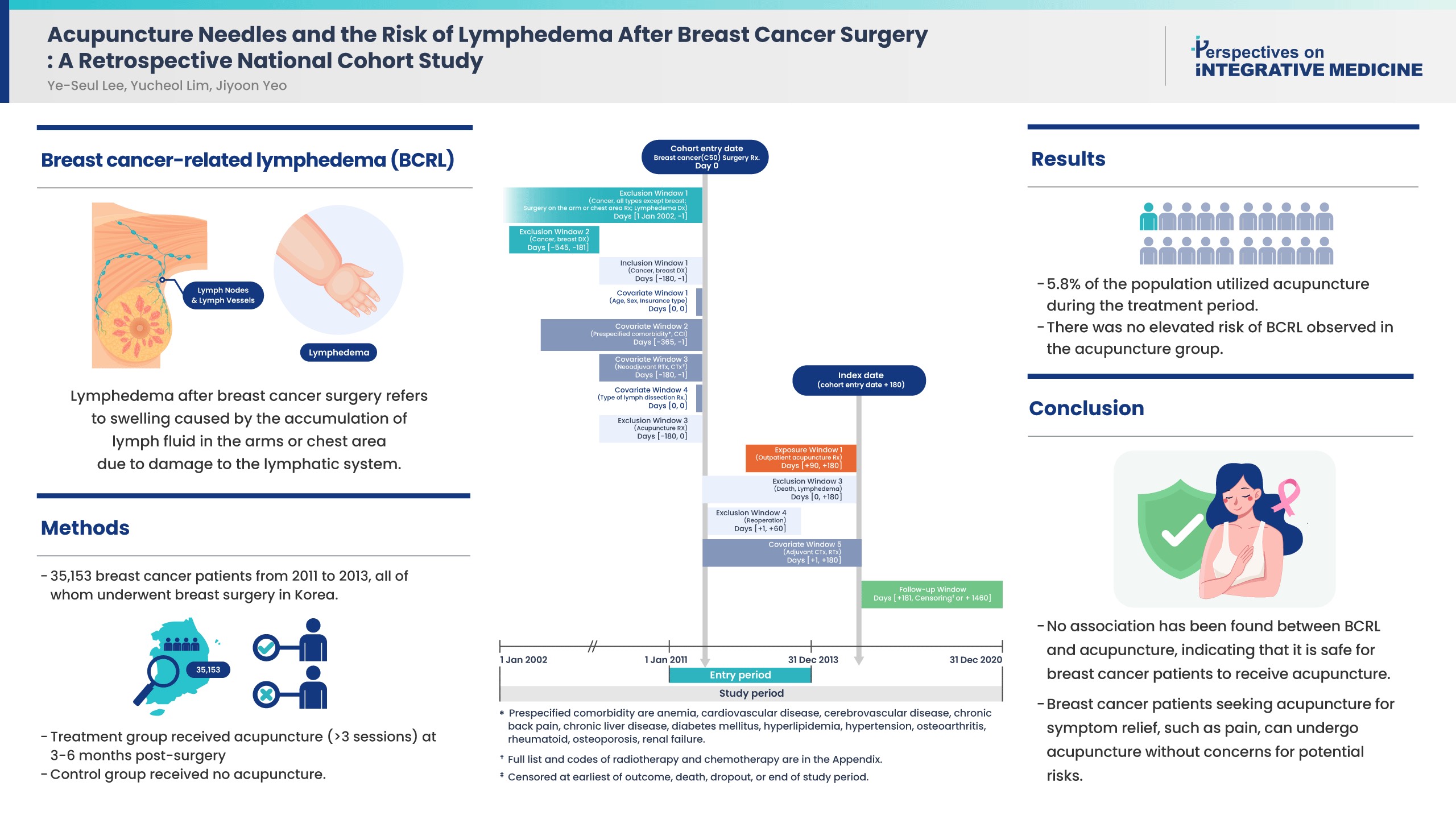
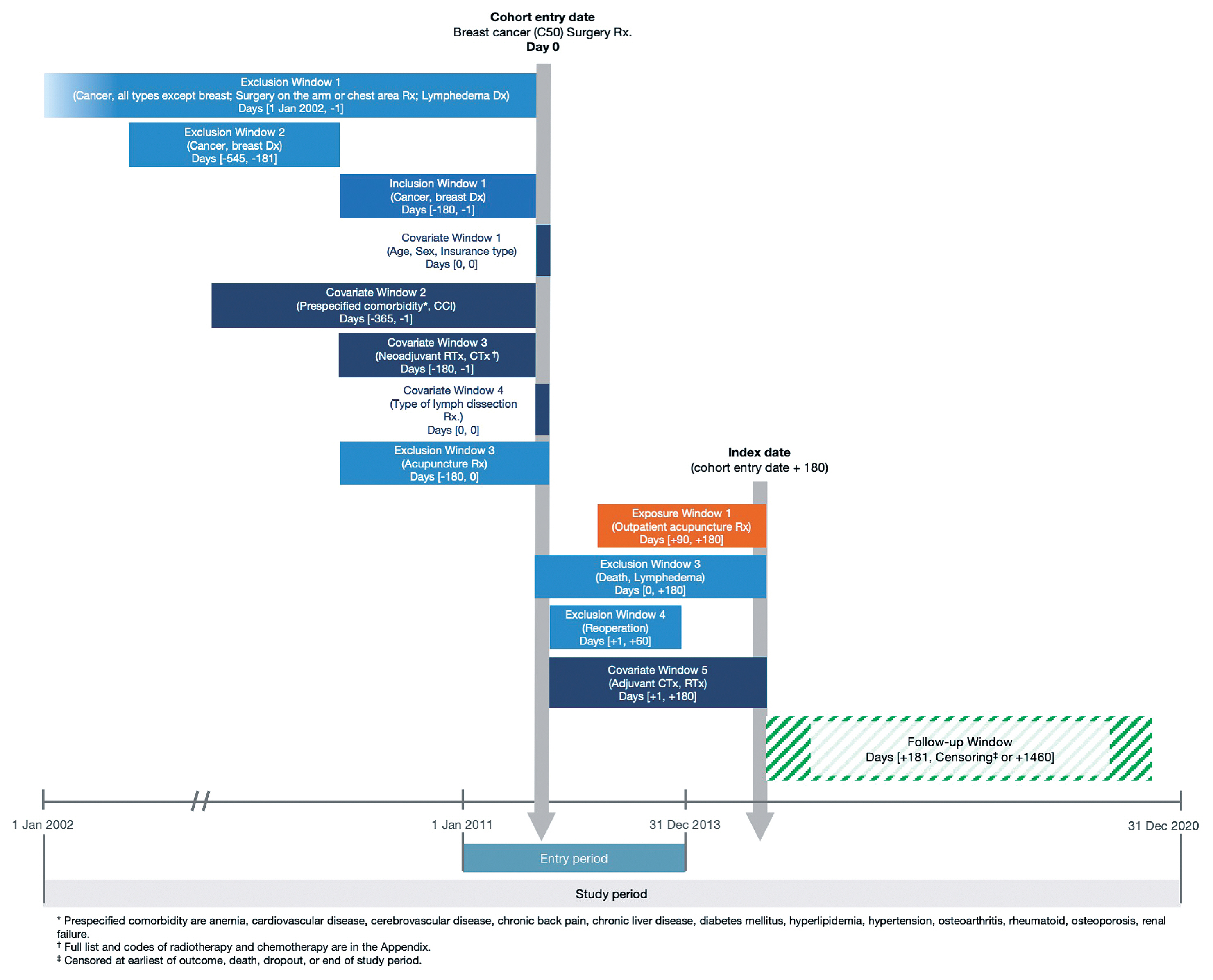
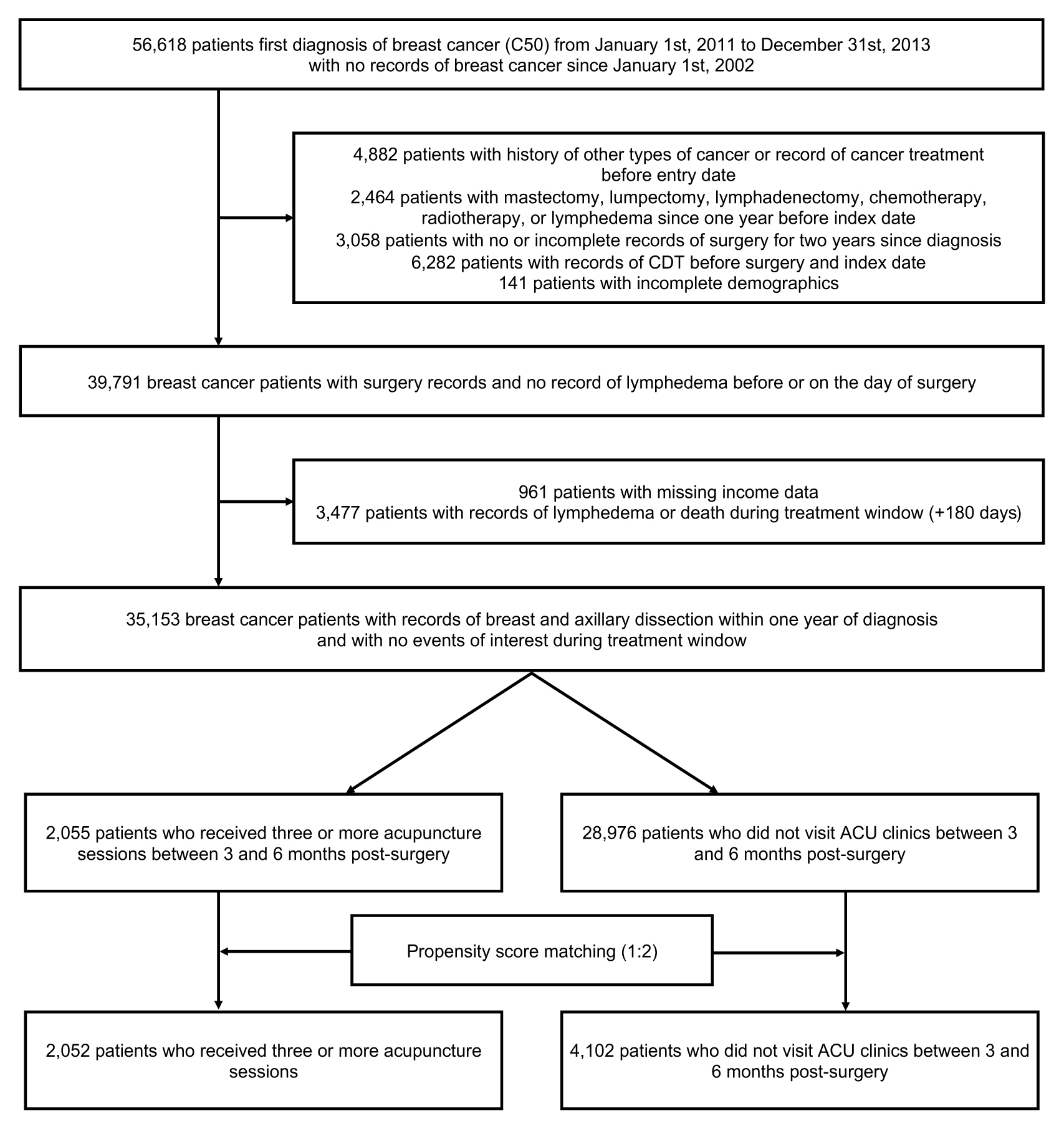
- The methodological approach of this study was designed to emulate a pragmatic clinical trial [19] to assess the influence of acupuncture treatments, in the months following breast cancer surgery, on the risk of BCRL (Fig. 1). Breast cancer patients newly diagnosed using the ICD-10 (International Classification of Diseases, 10th revision) code C50 from January 1, 2011 to December 31, 2013, and those who received a mastectomy or lumpectomy with axillary dissections were included in this study (Fig. 2). The exclusion criteria included: (1) history of any type of cancer since 2002; (2) surgical records of a mastectomy, lumpectomy, or lymphadenectomy before diagnosis; (3) no records of surgeries for more than 1 year after the diagnosis; (4) records of a lymphadenectomy without record of a mastectomy or lumpectomy; (5) diagnosis of BCRL before a breast cancer diagnosis, before surgery, or on the day of surgery; (6) record of complete decongestive therapy before diagnosis, before surgery, or on the day of surgery, and (7) no records of acupuncture treatment since the diagnosis and before the exposure window.
- 3. Intervention
- The target intervention of this study was defined using the reimbursement records from the NHIS database for acupuncture and/or electroacupuncture conducted at Korean medicine (KM) hospitals and clinics. A minimum of 5 sessions of acupuncture between 3–6 months after breast surgery or at least 1 acupuncture session per month were the factors used to define a patient as having received acupuncture treatment during the subacute postsurgical stage. Patients without records of visiting KM clinics were defined as the control group.
- 4. Outcome and covariates
- The outcome of this study was the incidence of BCRL within 5 years of surgery. Covariates included baseline characteristics, demographic factors (sex, age group, and insurance type), comorbidities using the Charlson Comorbidity Index (CCI) in the 1-year period before the breast cancer diagnosis, and cancer treatments including chemotherapy, radiotherapy, and hormonal therapy.
- 5. Statistical analysis
- Descriptive analysis was conducted to identify the baseline characteristics of the cohort. The propensity score was calculated as the probability of the patient receiving acupuncture after breast and axillary dissection. Classification variables in the propensity score calculation were demographics, type of breast and axillary dissection, neoadjuvant and adjuvant radiotherapy cycles, neoadjuvant and adjuvant chemotherapy cycles, CCI, and prespecified comorbid conditions. Propensity score matching (PSM) was applied using the greedy nearest neighbor method with 2 matched controls for each patient with a caliper of 0.1. The exact condition was applied for the type of breast and axillary dissection (sentinel lymph node biopsy or axillary lymph node dissection).
- Incidence rate ratio (IRR) and Cox proportional hazards models were employed to calculate the risk of BCRL. Four multivariable Cox regression models were generated to adjust for demographics, CCI, and cancer treatments in addition to surgeries. A Kaplan-Meier curve was generated to estimate the duration from the cohort index date until the incidence of BCRL. A 2-sided p < 0.05 was considered significant. Statistical analyses were conducted using the SAS Version 9.4 (SAS Institute, Cary, NC).
- 6. Sensitivity analysis
- Sensitivity analyses were conducted to verify the robustness of the results against adjustments in the operational definitions. Firstly, survival analyses were conducted on the cohort before PSM to examine the risk on the nationwide population. Secondly, the exposure window during the postsurgical stage was extended from was extended from 3–6 months post-surgery to 1–6 months post-surgery to reflect acupuncture treatments during the acute postsurgical stage. Thirdly, prespecified comorbidities in the 1-year period prior to a breast cancer diagnosis were adjusted for as covariates in the survival analyses instead of using the CCI. The prespecified comorbidities were: anemia, anxiety disorders, cardiovascular diseases, cerebrovascular disease, chronic back pain, chronic liver diseases, chronic obstructive pulmonary disease, dementia including Alzheimer’s, depressive disorders, diabetes mellitus, hyperlipidemia, hypertension, osteoarthritis, osteoporosis, renal failure, rheumatoid arthritis, schizophrenia, and sleep disorder (Supplementary Table 1).
Materials and Methods
- 1. Patient characteristics
- Among the 56,618 patients who were first diagnosed with breast cancer between 2011 and 2013, a total of 35,153 patients met the inclusion criteria and received breast and axillary dissection (Fig. 1). Among them, 2,055 patients (5.8%) who received a minimum of 3 acupuncture treatment sessions during the 3–6 month-stage post-surgery were selected as the treatment group (ACU group), and 28,976 patients (82.4%) who did not receive acupuncture treatments or visit KM clinics/hospitals during this period were selected as the control group.
- Before PSM, patients in the ACU group were older and had higher CCI scores than patients in the control group. ACU group patients had higher prevalence of chronic back pain (ACU: 44.0%, control: 24.6%), cardiovascular diseases (ACU: 4.2%, control: 2.8%), hypertension (ACU: 21.9%, control: 17.6%), osteoarthritis (ACU: 23.3%, control: 13.1%), osteoporosis (ACU: 6.5%, control: 3.9%), and sleep disorder (ACU: 4.1%, control: 2.1%). A higher number of patients in the ACU group received adjuvant radiotherapy (ACU: 57.2%, control: 51.4%), but a significantly smaller number in the ACU group received adjuvant chemotherapy (ACU: 37.8%, control: 64.1%), specifically, taxanes (ACU: 8.8%, control: 22.7%). Baseline characteristics of the cohort before matching is presented in Supplementary Table 2. After PSM, there were no significant difference in any of the aforementioned factors between 2 groups (Table 1). However, there were a significantly higher proportion of ACU group patients with CEVD (p < 0.048) and a lower percentage of ACU patients receiving adjuvant taxane treatments (p < 0.003; Table 1).
- 2. Risk of developing BCRL after receiving acupuncture treatments
- After PSM, the ACU group and the control group did not show statistical difference in the IRR of BCRL (IRR 1.017, 95% confidence interval (CI) 0.868–1.193, Supplementary Table 3). Survival analysis showed that the risk of BCRL in the ACU group was not significantly different from the control group (unadjusted HR 1.018, 95% CI 0.868–1.193, Supplementary Table 2). This risk remained robust, with no statistical significance between the AUC group and the control group using multivariate Cox proportional hazard models.
- 3. Sensitivity analysis
- Before PSM, the ACU group had significantly lower IRR of BCRL (IRR 0.822, 95% CI 0.720–0.940, Supplementary Table 4. Univariate survival analysis showed that ACU group had a slightly lower risk of BCRL than the control group (unadjusted hazard ratio (HR) 0.827, 95% CI 0.724–0.945, Supplementary Table 5). Adjusting for covariates in multivariate models yielded robust statistically insignificant hazard ratios. Application of the same study design to examine mortality showed statistically insignificant hazard ratios, implying there was no difference between the disease severity of the 2 groups (Supplementary Tables 3 and 4). The risk of lymphedema was consistent when comorbid conditions were adjusted (Supplementary Table 6).
- A new cohort was created when the operational definition of the postsurgical stage was modified to 1–6 months post-surgery. The survival analysis showed that the risk of BCRL of ACU group in the cohort after PSM was lower than the control group (unadjusted HR 0.858, 95% CI 0.744–0.990; Supplementary Table 7). The Kaplan-Meier curve showed no difference in the risk of BCRL between the ACU group and the control group (Supplementary Fig. 1). The risk was significantly lower in all multivariate Cox models. However, when PSM was applied, no difference in the risk of BCRL was observed between groups (unadjusted HR 1.087, 95% CI 0.903–1.310; Supplementary Table 7).
Results
- This article represents the first study to explore how acupuncture affects surgical complications in breast cancer patients, utilizing a nationwide cohort. While recent research indicates that restricting vascular access post-surgery to prevent BCRL may be unnecessary [5–7,20], the impact of acupuncture on BCRL risk has not been investigated. To address this pertinent clinical question and navigate the difficulties inherent in clinical trial design and execution in this area, our research assessed the effects of acupuncture during the subacute postoperative phase. Utilizing data from a national cohort, we observed no significant link between acupuncture and BCRL risk.
- Clinical guidelines for breast cancer patients, sometimes shaped by anecdotal evidence and concerns regarding complications, have historically advised against invasive therapies like acupuncture due to infection [6,21]. This caution regarding the use of needles limits the options for managing other issues, such as postmastectomy pain. The findings of this current study align with previous cohort studies showing no BCRL link with intravenous treatments [4,5]. We observed that acupuncture, initiated between 3 to 6 months post-surgery did not affect BCRL risk, a conclusion supported by sensitivity analysis even when acupuncture began as early as 1-month post-surgery.
- The study cohort was carefully selected to represent newly diagnosed Stage I/II breast cancer patients without history of lymphedema or related treatments, and with specific inclusion and exclusion criteria ensuring homogeneity. The acupuncture exposure window was confined to 3–6 months post-surgery. This selective approach may explain the cohort’s relatively low BCRL incidence rate (13%) and minimal uptake of acupuncture (5.8%) [22–24]. It has been reported that 25.5% of breast cancer patients in Korea [25] and 26% [26] to 52% [27] in other countries such as Sweden and Canada used acupuncture after surgery. Another study reported that 12.3% of breast cancer patients in the United States used acupuncture [28]. A broader inclusion of complementary and alternative medicine (CAM) therapies over an extended period may have shown higher utilization in our study.
- Before PSM, the ACU group of patients were generally older, with more comorbidities and a higher CCI, and more factors linked to increased use of CAM [29]. They also differed in their treatment approaches compared to the control group. These disparities necessitated cautious interpretation of the pre-PSM data regarding BCRL risk.
- Although patients often use acupuncture and CAM for various treatment-related complications such as post-mastectomy pain, arthralgia, hot flashes, and nausea and vomiting [28,30,31], this study’s scope did not extend to symptoms other than BCRL. A different study design is required to investigate acupuncture’s effects on chronic symptoms. A few studies have explored the effect of acupuncture on BCRL management [32–34], but analyzing the effect of acupuncture on BCRL management would also require a different study design.
- The study’s limitations include not identifying specific acupuncture sites, specific needling protocols such as alcohol swabbing, and not categorizing chemotherapy, and endocrine therapy regimens. As patients likely underwent chemotherapy concurrently with acupuncture, further research is needed to explore the interactions between acupuncture and cancer therapies. Another limitation of the study was the scope of acupuncture treatments were not restricted, thus, allowing a potentially wide range of acupuncture applications and locations. Further study is required to examine the specific effect of acupuncture treatment details such as location, cleansing, and needling depth on the risk of BCRL.
- In summary, the findings of this study suggest that acupuncture treatment during the subacute postsurgical stage for symptom management such as pain, does not increase BCRL risk. This supports the safe use of acupuncture by breast cancer patients to address complications related to anticancer treatments.
Discussion
Supplementary Material
Acknowledgments
-
Author Contributions
YSL conceptualized the study design, acquired the data, interpreted the results, and wrote the manuscript. YCL and YJL reviewed the study design, acquired the data, and performed the statistical analyses. IHH revised and approved the final manuscript.
-
Conflicts of Interest
Ye-Seul Lee is an associate editor of Perspectives on Integrative Medicine however, this did not influence the journal’s decision to publish this article. All other authors state that there was no conflict of interest.
-
Funding
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, funded by the Ministry of Health and Welfare, Republic of Korea (no.: HF20C0222). The funders had no role in any part of this study.
-
Ethical Statement
The Institutional Review Board of Gachon University (no.: 1044396-202101-HR-001-01) approved this retrospective cohort study and waived informed consent because the patients were de-identified. This study was performed in accordance with the Declaration of Helsinki and relevant guidelines and regulations.
Article information
Data Availability
| Variables | 2:1 Propensity score matching | p | |||
|---|---|---|---|---|---|
| Non-ACU group (n = 4,102) | ACU group* (n = 2,052) | ||||
| N | % | N | % | ||
| Sex | 0.8702 | ||||
| Female | 4,089 | 99.7 | 2,046 | 99.7 | |
|
|
|||||
| Age groups (y) | 0.849 | ||||
| < 35 | 116 | 2.8 | 62 | 3.0 | |
| 35–44 | 769 | 18.8 | 386 | 18.8 | |
| 45–54 | 1,502 | 36.6 | 744 | 36.3 | |
| 55–64 | 838 | 20.4 | 397 | 19.4 | |
| 65–74 | 631 | 15.4 | 343 | 16.7 | |
| 75–84 | 235 | 5.7 | 114 | 5.6 | |
| ≥ 85 | 11 | 0.3 | 6 | 0.3 | |
|
|
|||||
| Insurance type | 0.755 | ||||
| NHI | 3,933 | 95.9 | 1,964 | 95.7 | |
| Medical Aid | 169 | 4.1 | 88 | 4.3 | |
|
|
|||||
| CCI | 0.396 | ||||
| 0 | 3,367 | 82.1 | 1,656 | 80.7 | |
| 1–2 | 589 | 14.4 | 314 | 15.3 | |
| 3- | 146 | 3.6 | 82 | 4.0 | |
|
|
|||||
| Income quintile | 0.821 | ||||
| 1st | 169 | 4.1 | 88 | 4.3 | |
| 2nd | 662 | 16.1 | 353 | 17.2 | |
| 3rd | 698 | 17.0 | 334 | 16.3 | |
| 4th | 907 | 22.1 | 450 | 21.9 | |
| 5th | 1,666 | 40.6 | 827 | 40.3 | |
|
|
|||||
| Operation type | 0.998 | ||||
| SLNB | 834 | 20.3 | 417 | 20.3 | |
| ALND | 3,205 | 78.1 | 1,603 | 78.1 | |
| Reoperation within 2-month | 63 | 1.54 | 32 | 1.6 | |
|
|
|||||
| Neoadjuvant chemotherapy | 0.769 | ||||
| Yes | 618 | 15.1 | 315 | 15.4 | |
| No. of sessions | 0.786 | ||||
| 0 | 3,484 | 84.9 | 1,737 | 84.7 | |
| 1–3 | 250 | 6.1 | 138 | 6.7 | |
| 4–6 | 364 | 8.9 | 175 | 8.5 | |
| 7–9 | 4 | 0.1 | 2 | 0.1 | |
|
|
|||||
| Comorbid conditions† | |||||
| Anemia | 108 | 2.6 | 59 | 2.9 | 0.581 |
| Anxiety disorder | 115 | 2.8 | 67 | 3.3 | 0.314 |
| CBP | 1,784 | 43.5 | 902 | 44.0 | 0.728 |
| CEVD | 100 | 2.4 | 68 | 3.3 | 0.048 |
| CLD | 142 | 3.5 | 77 | 3.8 | 0.562 |
| COPD | 24 | 0.6 | 12 | 0.6 | 0.999 |
| CVD | 141 | 3.4 | 86 | 4.2 | 0.139 |
| Dementia | 25 | 0.6 | 8 | 0.4 | 0.266 |
| Depressive disorder | 104 | 2.5 | 55 | 2.7 | 0.735 |
| DM | 297 | 7.2 | 164 | 8.0 | 0.291 |
| HL | 273 | 6.7 | 134 | 6.5 | 0.852 |
| HTN | 887 | 21.6 | 449 | 21.9 | 0.817 |
| OA | 944 | 23.0 | 477 | 23.3 | 0.838 |
| OSP | 270 | 6.6 | 132 | 6.4 | 0.823 |
| RA | 70 | 1.7 | 37 | 1.8 | 0.785 |
| RF | 22 | 0.5 | 11 | 0.5 | 0.999 |
| Schizophrenia | 15 | 0.4 | 2 | 0.1 | 0.059 |
| Sleep disorder | 151 | 3.7 | 83 | 4.0 | 0.482 |
|
|
|||||
| Adjuvant radiotherapy‡ | 0.514 | ||||
| Yes | 2,313 | 56.4 | 1,175 | 57.3 | |
| No. of sessions | 0.300 | ||||
| 0 | 1,789 | 43.6 | 877 | 42.7 | |
| 1–10 | 553 | 13.5 | 245 | 11.9 | |
| 11–20 | 120 | 2.9 | 59 | 2.9 | |
| 21–30 | 706 | 17.2 | 370 | 18.0 | |
| 31– | 934 | 22.8 | 501 | 24.4 | |
|
|
|||||
| Adjuvant chemotherapy‡ | 0.612 | ||||
| Yes | 1,522 | 37.1 | 775 | 37.8 | |
| No. of sessions | 0.907 | ||||
| 0 | 2,580 | 62.9 | 1,277 | 62.2 | |
| 1–3 | 184 | 4.5 | 99 | 4.8 | |
| 4–6 | 782 | 19.1 | 396 | 19.3 | |
| 7–9 | 408 | 10.0 | 212 | 10.3 | |
| 10- | 148 | 3.6 | 68 | 3.3 | |
|
|
|||||
| Adjuvant taxane treatments‡ | 0.003 | ||||
| Yes | 462 | 11.3 | 180 | 8.8 | |
|
|
|||||
| Outcomes | |||||
| Lymphedema | 450 | 11.0 | 229 | 11.2 | 0.823 |
| Death within 4-year follow-up | 139 | 3.4 | 72 | 3.5 | 0.807 |
* ACU group was defined by 3 or more sessions of acupuncture during 3–6 months post-surgery period.
† Prespecified comorbid conditions 1 year before the onset.
‡ Followed up until incidence of lymphedema or until the completion of the 4-year follow-up.
ACU = acupuncture; NHI = National Health Insurance; CCI = Charlson Comorbidity Index; SLNB = sentinel lymph node biopsy; ALND = axillary lymph node dissection; CBP = chronic low back pain; CEVD = cerebrovascular disease; CLD = chronic liver disease; COPD = chronic obstructive pulmonary disease; CVD = cardiovascular disease; DM = diabetes mellitus; HL = hyperlipidemia; HTN = hypertension; OA = osteoarthritis; OSP = osteoporosis; RA = rheumatic arthritis; RF = renal failure.
- [1] Fish ML, Grover R, Schwarz GS. Quality-of-life outcomes in surgical vs nonsurgical treatment of breast cancer-related lymphedema: a systematic review. JAMA Surg 2020;155(6):513−9.ArticlePubMed
- [2] Armer JM, Ballman KV, McCall L, Ostby PL, Zagar E, Kuerer HM, et al. Factors associated with lymphedema in women with node-positive breast cancer treated with neoadjuvant chemotherapy and axillary dissection. JAMA Surg 2019;154(9):800−9.ArticlePubMedPMC
- [3] Sakorafas GH, Peros G, Cataliotti L, Vlastos G. Lymphedema following axillary lymph node dissection for breast cancer. Surg Oncol 2006;15(3):153−65.ArticlePubMed
- [4] Kilbreath SL, Refshauge KM, Beith JM, Ward LC, Ung OA, Dylke ES, et al. Risk factors for lymphoedema in women with breast cancer: A large prospective cohort. Breast 2016;28:29−36.ArticlePubMed
- [5] Ferguson CM, Swaroop MN, Horick N, Skolny MN, Miller CL, Jammallo LS, et al. Impact of ipsilateral blood draws, injections, blood pressure measurements, and air travel on the risk of lymphedema for patients treated for breast cancer. J Clin Oncol 2016;34(7):691−8.ArticlePubMedPMC
- [6] Larocque G, McDiarmid S. The legacy of lymphedema: Impact on nursing practice and vascular access. Can Oncol Nurs J 2019;29(3):194−203.PubMedPMC
- [7] McDiarmid S, Larocque G. Time to rethink vascular access in patients with breast cancer. Br J Nurs 2020;29(14):S32−8.Article
- [8] Deng G, Vickers A, Yeung S, D’Andrea GM, Xiao H, Heerdt AS, et al. Randomized, controlled trial of acupuncture for the treatment of hot flashes in breast cancer patients. J Clin Oncol 2007;25(35):5584−90.ArticlePubMed
- [9] Frisk J, Carlhall S, Kallstrom AC, Lindh-Astrand L, Malmstrom A, Hammar M. Long-term follow-up of acupuncture and hormone therapy on hot flushes in women with breast cancer: a prospective, randomized, controlled multicenter trial. Climacteric 2008;11(2):166−74.ArticlePubMed
- [10] Hervik J, Mjaland O. Acupuncture for the treatment of hot flashes in breast cancer patients, a randomized, controlled trial. Breast Cancer Res Treat 2009;116(2):311−6.ArticlePubMedPDF
- [11] Collins KB, Thomas DJ. Acupuncture and acupressure for the management of chemotherapy-induced nausea and vomiting. J Am Acad Nurse Pract 2004;16(2):76−80.ArticlePubMed
- [12] Greenlee H, DuPont-Reyes MJ, Balneaves LG, Carlson LE, Cohen MR, Deng G, et al. Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J Clin 2017;67(3):194−232.ArticlePubMedPMCPDF
- [13] Yang Y, Zhang Y, Jing NC, Lu Y, Xiao HY, Xu GL, et al. Electroacupuncture at Zusanli (ST 36) for treatment of nausea and vomiting caused by the chemotherapy of the malignant tumor: a multicentral randomized controlled trial. Zhongguo Zhen Jiu 2009;29(12):955−8. [in Chinese].PubMed
- [14] Liu X, Lu J, Wang G, Chen X, Xv H, Huang J, et al. Acupuncture for arthralgia induced by aromatase inhibitors in patients with breast cancer: a systematic review and meta-analysis. Integr Cancer Ther 2021;20:1534735420980811. ArticlePubMedPMCPDF
- [15] Lu W, Giobbie-Hurder A, Freedman RA, Shin IH, Lin NU, Partridge AH, et al. Acupuncture for chemotherapy-induced peripheral neuropathy in breast cancer survivors: a randomized controlled pilot trial. Oncologist 2020;25(4):310−8.ArticlePubMedPMCPDF
- [16] Health Insurance Review and Accessment Service [Internet]. 2020 national health insurance statistical yearbook: 2020 Available from: https://www.hira.or.kr/bbsDummy.do?pgmid=HIRAJ030000007001&brdScnBltNo=4&brdBltNo=3#none [in Korean]
- [17] Kim S, Kim MS, You SH, Jung SY. Conducting and reporting a clinical research using Korean healthcare claims database. Korean J Fam Med 2020;41(3):146−52. [in Korean].ArticlePubMedPMCPDF
- [18] Seong SC, Kim YY, Khang YH, Heon Park J, Kang HJ, Lee H, et al. Data resource profile: the national health information database of the national health insurance service in south Korea. Int J Epidemiol 2017;46(3):799−800.PubMed
- [19] Hernan MA, Robins JM. Using big data to emulate a target trial when a randomized trial is not available. Am J Epidemiol 2016;183(8):758−64.ArticlePubMedPMC
- [20] Yao C, Xu Y, Chen L, Jiang H, Ki CS, Byun JS, et al. Effects of warm acupuncture on breast cancer-related chronic lymphedema: a randomized controlled trial. Curr Oncol 2016;23(1):e27−34..ArticlePubMedPMC
- [21] Cheng CT, Deitch JM, Haines IE, Porter DJ, Kilbreath SL. Do medical procedures in the arm increase the risk of lymphoedema after axillary surgery? A review. ANZ J Surg 2014;84(7–8):510−4.ArticlePubMed
- [22] DiSipio T, Rye S, Newman B, Hayes S. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol 2013;14(6):500−15.ArticlePubMed
- [23] Zou L, Liu FH, Shen PP, Hu Y, Liu XQ, Xu YY, et al. The incidence and risk factors of related lymphedema for breast cancer survivors post-operation: a 2-year follow-up prospective cohort study. Breast Cancer 2018;25(3):309−14.ArticlePubMedPDF
- [24] Shen A, Lu Q, Fu X, Wei X, Zhang L, Bian J, et al. Risk factors of unilateral breast cancer-related lymphedema: an updated systematic review and meta-analysis of 84 cohort studies. Support Care Cancer 2022;31(1):18. ArticlePubMedPDF
- [25] Kim D, Sung SH, Shin S, Park M. The effect of cancer on traditional, complementary and alternative medicine utilization in Korea: a fixed effect analysis using Korea Health Panel data. BMC Complement Med Ther 2022;22(1):137. ArticlePubMedPMCPDF
- [26] Wode K, Henriksson R, Sharp L, Stoltenberg A, Hok Nordberg J. Cancer patients’ use of complementary and alternative medicine in Sweden: a cross-sectional study. BMC Complement Altern Med 2019;19(1):62. ArticlePubMedPMCPDF
- [27] Buckner CA, Lafrenie RM, Denommee JA, Caswell JM, Want DA. Complementary and alternative medicine use in patients before and after a cancer diagnosis. Curr Oncol 2018;25(4):e275−81..ArticlePubMedPMCPDF
- [28] Zayas J, Ruddy KJ, Olson JE, Couch FJ, Bauer BA, Mallory MJ, et al. Real-world experiences with acupuncture among breast cancer survivors: a cross-sectional survey study. Support Care Cancer 2020;28(12):5833−8.ArticlePubMedPMCPDF
- [29] Lee Y-S, Lee I-S, Kim S-Y, Lee H, Park H-J, Lee H, et al. Identification of determinants of the utilisation of acupuncture treatment using Andersen’s behavioural model. Acupunct Med 2015;33(2):129−35.ArticlePubMedPDF
- [30] Jang S, Ko Y, Sasaki Y, Park S, Jo J, Kang NH, et al. Acupuncture as an adjuvant therapy for management of treatment-related symptoms in breast cancer patients: systematic review and meta-analysis (PRISMA-compliant). Medicine (Baltimore) 2020;99(50):e21820. PubMedPMC
- [31] Han G, Lee YS, Jang HJ, Kim SY, Lee YJ, Ha IH. Symptom management and quality of life of breast cancer patients using acupuncture-related therapies and herbal medicine: a scoping review. Cancers (Basel) 2022;14(19):4683. ArticlePubMedPMC
- [32] Cassileth BR, Van Zee KJ, Yeung KS, Coleton MI, Cohen S, Chan YH, et al. Acupuncture in the treatment of upper-limb lymphedema: results of a pilot study. Cancer 2013;119(13):2455−61.ArticlePubMedPMCPDF
- [33] Jeong YJ, Kwon HJ, Park YS, Kwon OC, Shin IH, Park SH. Treatment of lymphedema with saam acupuncture in patients with breast cancer: a pilot study. Med Acupunct 2015;27(3):206−15.ArticlePubMedPMC
- [34] Bao T, Iris Zhi W, Vertosick EA, Li QS, DeRito J, Vickers A, et al. Acupuncture for breast cancer-related lymphedema: a randomized controlled trial. Breast Cancer Res Treat 2018;170(1):77−87.ArticlePubMedPMCPDF
References
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite